Hemicorporectomy is a radical surgery in which the body below the waist is amputated, transecting the lumbar spine. This removes the legs, the genitalia, urinary system, pelvic bones, anus, and rectum. It is a major procedure recommended only as a last resort for people with severe and potentially fatal illnesses such as osteomyelitis, tumors, severe traumas and intractable decubiti in, or around, the pelvis. By 2009, 66 cases had been reported in medical literature.

Airway management includes a set of maneuvers and medical procedures performed to prevent and relieve airway obstruction. This ensures an open pathway for gas exchange between a patient's lungs and the atmosphere. This is accomplished by either clearing a previously obstructed airway; or by preventing airway obstruction in cases such as anaphylaxis, the obtunded patient, or medical sedation. Airway obstruction can be caused by the tongue, foreign objects, the tissues of the airway itself, and bodily fluids such as blood and gastric contents (aspiration).

Major trauma is any injury that has the potential to cause prolonged disability or death. There are many causes of major trauma, blunt and penetrating, including falls, motor vehicle collisions, stabbing wounds, and gunshot wounds. Depending on the severity of injury, quickness of management, and transportation to an appropriate medical facility may be necessary to prevent loss of life or limb. The initial assessment is critical, and involves a physical evaluation and also may include the use of imaging tools to determine the types of injuries accurately and to formulate a course of treatment.

Clearing the cervical spine is the process by which medical professionals determine whether cervical spine injuries exist, mainly regarding cervical fracture. It is generally performed in cases of major trauma. This process can take place in the emergency department or in the field by appropriately trained EMS personnel.

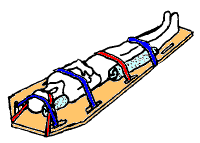
A vacuum mattress, or vacmat, is a medical device used for the immobilisation of patients, especially in case of a vertebra, pelvis or limb trauma. It is also used for manual transportation of patients for short distances. It was invented by Loed and Haederlé, who called it "shell" mattress.
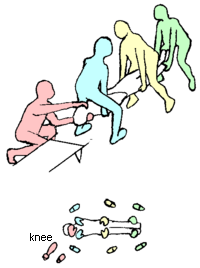
Casualty lifting is the first step of casualty movement, an early aspect of emergency medical care. It is the procedure used to put the casualty on a stretcher.

Vehicle extrication is the process of removing a patient from a vehicle which has been involved in a motor vehicle collision. Patients who have not already exited a crashed vehicle may be medically or physically trapped, and may be pinned by wreckage, or unable to exit the vehicle because a door will not open.

A spinal cord injury (SCI) is damage to the spinal cord that causes temporary or permanent changes in its function. It is a destructive neurological and pathological state that causes major motor, sensory and autonomic dysfunctions.

A cervical collar, also known as a neck brace, is a medical device used to support and immobilize a person's neck. It is also applied by emergency personnel to those who have had traumatic head or neck injuries, although they should not be routinely used in prehospital care. They can also be used to treat chronic medical conditions.

A Kendrick extrication device (KED) is a device used in extrication of victims of traffic collisions from motor vehicles. Commonly carried on ambulances, a KED is typically used by an emergency medical technician, paramedic, or another first responder. It was originally designed for extrication of race car drivers. Typically used in conjunction with a cervical collar, a KED is a semi-rigid brace that secures the head, neck and torso in an anatomically neutral position. Its use is claimed to reduce the possibility of additional injuries to these regions during extrication, although its value has been questioned, as there is a lack of evidence to support its use. The original KED was designed by Richard Kendrick in 1978.

The scoop stretcher is a device used specifically for moving injured people. It is ideal for carrying casualties with possible spinal injuries.

A cervical fracture, commonly called a broken neck, is a fracture of any of the seven cervical vertebrae in the neck. Examples of common causes in humans are traffic collisions and diving into shallow water. Abnormal movement of neck bones or pieces of bone can cause a spinal cord injury, resulting in loss of sensation, paralysis, or usually death soon thereafter, primarily via compromising neurological supply to the respiratory muscles and innervation to the heart.

Advanced trauma life support (ATLS) is a training program for medical providers in the management of acute trauma cases, developed by the American College of Surgeons. Similar programs exist for immediate care providers such as paramedics. The program has been adopted worldwide in over 60 countries, sometimes under the name of Early Management of Severe Trauma, especially outside North America. Its goal is to teach a simplified and standardized approach to trauma patients. Originally designed for emergency situations where only one doctor and one nurse are present, ATLS is now widely accepted as the standard of care for initial assessment and treatment in trauma centers. The premise of the ATLS program is to treat the greatest threat to life first. It also advocates that the lack of a definitive diagnosis and a detailed history should not slow the application of indicated treatment for life-threatening injury, with the most time-critical interventions performed early.
A traction splint most commonly refers to a splinting device that uses straps attaching over the pelvis or hip as an anchor, a metal rod(s) to mimic normal bone stability and limb length, and a mechanical device to apply traction to the limb.
Stabilization is a process to help prevent a sick or injured person from having their medical condition deteriorate further so that they can be treated. Examples include while the person is waiting for medical treatment and in the intensive care unit.
Whole body vibration (WBV) is a generic term used when vibrations (mechanical oscillations) of any frequency are transferred to the human body. Humans are exposed to vibration through a contact surface that is in a mechanical vibrating state. Humans are generally exposed to many different forms of vibration in their daily lives. This could be through a driver's seat, a moving train platform, a power tool, a training platform, or any one of countless other devices. It is a potential form of occupational hazard, particularly after years of exposure.
Grady straps are a specific strapping configuration used in full body spinal immobilization.

In sports medicine, helmet removal is the practice of removing the helmet of someone who has just experienced a sports injury in order to better facilitate first aid. Obvious causes include head and neck injury, or both, with no immediate means of excluding neck injury in the athlete who may be unable to give a history.

Airtraq is a fibreoptic intubation device used for indirect tracheal intubation in difficult airway situations. It is designed to enable a view of the glottic opening without aligning the oral with the pharyngeal, and laryngeal axes as an advantage over direct endotracheal intubation and allows for intubation with minimal head manipulation and positioning.

Spinal precautions, also known as spinal immobilization and spinal motion restriction, are efforts to prevent movement of the bones of the spine in those with a risk of a spine injury. This is done as an effort to prevent injury to the spinal cord in unstable spinal fractures. About 0.5-3% of people with blunt trauma will have a spine injury, with 42-50% of injuries due to motor vehicle accidents, 27-43% from falls or work injuries, and the rest due to sports injuries (9%) or assault (11%). The majority of spinal cord injuries are to the cervical spine, followed by the thoracic and lumbar spine. Cervical spinal cord injuries can result in tetraplegia or paraplegia, depending on severity. Of spine injuries, only 0.01% are unstable and require intervention.