Related Research Articles

The trachea, also known as the windpipe, is a cartilaginous tube that connects the larynx to the bronchi of the lungs, allowing the passage of air, and so is present in almost all animals with lungs. The trachea extends from the larynx and branches into the two primary bronchi. At the top of the trachea the cricoid cartilage attaches it to the larynx. The trachea is formed by a number of horseshoe-shaped rings, joined together vertically by overlying ligaments, and by the trachealis muscle at their ends. The epiglottis closes the opening to the larynx during swallowing.

Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic tube into the trachea (windpipe) to maintain an open airway or to serve as a conduit through which to administer certain drugs. It is frequently performed in critically injured, ill, or anesthetized patients to facilitate ventilation of the lungs, including mechanical ventilation, and to prevent the possibility of asphyxiation or airway obstruction.
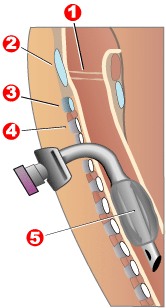
Tracheotomy, or tracheostomy, is a surgical airway management procedure which consists of making an incision (cut) on the anterior aspect (front) of the neck and opening a direct airway through an incision in the trachea (windpipe). The resulting stoma (hole) can serve independently as an airway or as a site for a tracheal tube or tracheostomy tube to be inserted; this tube allows a person to breathe without the use of the nose or mouth.
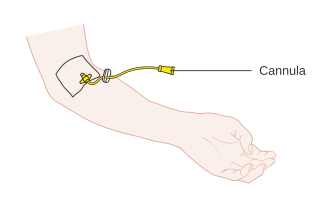
A cannula is a tube that can be inserted into the body, often for the delivery or removal of fluid or for the gathering of samples. In simple terms, a cannula can surround the inner or outer surfaces of a trocar needle thus extending the effective needle length by at least half the length of the original needle. Its size mainly ranges from 14 to 26 gauge. Different-sized cannula have different colours as coded.
A tracheal tube is a catheter that is inserted into the trachea for the primary purpose of establishing and maintaining a patent airway and to ensure the adequate exchange of oxygen and carbon dioxide.
Airway management includes a set of maneuvers and medical procedures performed to prevent and relieve airway obstruction. This ensures an open pathway for gas exchange between a patient's lungs and the atmosphere. This is accomplished by either clearing a previously obstructed airway; or by preventing airway obstruction in cases such as anaphylaxis, the obtunded patient, or medical sedation. Airway obstruction can be caused by the tongue, foreign objects, the tissues of the airway itself, and bodily fluids such as blood and gastric contents (aspiration).

Respiratory arrest is a serious medical condition caused by apnea or respiratory dysfunction severe enough that it will not sustain the body. Prolonged apnea refers to a patient who has stopped breathing for a long period of time. If the heart muscle contraction is intact, the condition is known as respiratory arrest. An abrupt stop of pulmonary gas exchange lasting for more than five minutes may permanently damage vital organs, especially the brain. Lack of oxygen to the brain causes loss of consciousness. Brain injury is likely if respiratory arrest goes untreated for more than three minutes, and death is almost certain if more than five minutes.

A peripherally inserted central catheter, less commonly called a percutaneous indwelling central catheter, is a form of intravenous access that can be used for a prolonged period of time or for administration of substances that should not be done peripherally. It is a catheter that enters the body through the skin (percutaneously) at a peripheral site, extends to the superior vena cava, and stays in place for days, weeks or even months.
Stridor is a high-pitched extra-thoracic breath sound resulting from turbulent air flow in the larynx or lower in the bronchial tree. It is different from a stertor which is a noise originating in the pharynx.

A cricothyrotomy is an incision made through the skin and cricothyroid membrane to establish a patent airway during certain life-threatening situations, such as airway obstruction by a foreign body, angioedema, or massive facial trauma. Cricothyrotomy is nearly always performed as a last resort in cases where other means of tracheal intubation are impossible or impractical. Compared with tracheotomy, cricothyrotomy is quicker and easier to perform, does not require manipulation of the cervical spine, and is associated with fewer complications. However, while cricothyrotomy may be life-saving in extreme circumstances, this technique is only intended to be a temporizing measure until a definitive airway can be established.
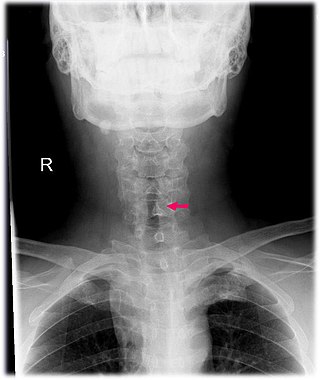
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway. It can be congenital, acquired, iatrogenic, or very rarely, idiopathic. It is defined as the narrowing of the portion of the airway that lies between the vocal cords and the lower part of the cricoid cartilage. In a normal infant, the subglottic airway is 4.5-5.5 millimeters wide, while in a premature infant, the normal width is 3.5 millimeters. Subglottic stenosis is defined as a diameter of under 4 millimeters in an infant. Acquired cases are more common than congenital cases due to prolonged intubation being introduced in the 1960s. It is most frequently caused by certain medical procedures or external trauma, although infections and systemic diseases can also cause it.

Bronchoscopy is an endoscopic technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. An instrument (bronchoscope) is inserted into the airways, usually through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs. The construction of bronchoscopes ranges from rigid metal tubes with attached lighting devices to flexible optical fiber instruments with realtime video equipment.
Following is a list of instruments used in the practice of anesthesia

Tracheobronchial injury is damage to the tracheobronchial tree. It can result from blunt or penetrating trauma to the neck or chest, inhalation of harmful fumes or smoke, or aspiration of liquids or objects.

Urethrostomy is a surgical procedure that creates a permanent opening in the urethra, commonly to remove obstructions to urine flow. The procedure is most often performed in male cats, where the opening is made in the perineum.
Cholecystostomy is a procedure where a stoma is created in the gallbladder, which can facilitate placement of a tube for drainage, first performed by American surgeon, Dr. John Stough Bobbs, in 1867. It is sometimes used in cases of cholecystitis where the person is ill, and there is a need to delay or defer cholecystectomy. The first endoscopic cholecystostomy was performed by Drs. Todd Baron and Mark Topazian in 2007 using ultrasound guidance to puncture the stomach wall and place a plastic biliary catheter for gallbladder drainage.
Tracheal intubation, an invasive medical procedure, is the placement of a flexible plastic catheter into the trachea. For millennia, tracheotomy was considered the most reliable method of tracheal intubation. By the late 19th century, advances in the sciences of anatomy and physiology, as well as the beginnings of an appreciation of the germ theory of disease, had reduced the morbidity and mortality of this operation to a more acceptable rate. Also in the late 19th century, advances in endoscopic instrumentation had improved to such a degree that direct laryngoscopy had finally become a viable means to secure the airway by the non-surgical orotracheal route. Nasotracheal intubation was not widely practiced until the early 20th century. The 20th century saw the transformation of the practices of tracheotomy, endoscopy and non-surgical tracheal intubation from rarely employed procedures to essential components of the practices of anesthesia, critical care medicine, emergency medicine, gastroenterology, pulmonology and surgery.

Surgical airway management is the medical procedure ensuring an open airway between a patient’s lungs and the outside world. Surgical methods for airway management rely on making a surgical incision below the glottis in order to achieve direct access to the lower respiratory tract, bypassing the upper respiratory tract. Surgical airway management is often performed as a last resort in cases where orotracheal and nasotracheal intubation are impossible or contraindicated. Surgical airway management is also used when a person will need a mechanical ventilator for a longer period. The surgical creation of a permanent opening in the larynx is referred to as laryngostomy. Surgical airway management is a primary consideration in anaesthesia, emergency medicine and intensive care medicine.
Advanced airway management is the subset of airway management that involves advanced training, skill, and invasiveness. It encompasses various techniques performed to create an open or patent airway – a clear path between a patient's lungs and the outside world.
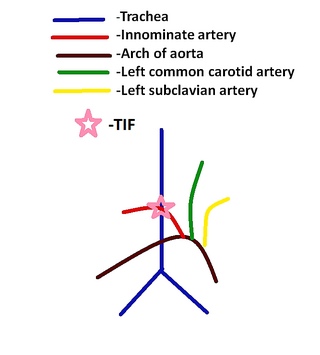
Tracheoinnominate fistula is an abnormal connection (fistula) between the innominate artery and the trachea. A TIF is a rare but life-threatening iatrogenic injury, usually the sequela of a tracheotomy.
References
- 1 2 Types of Tracheostomy Tubes. Aaron's Tracheostomy Page. 2004. Retrieved November 22, 2009.
- 1 2 3 Lindman, Jonathan. 2009. Tracheostomy. Department of Otolaryngology, ENT Care Associates.
- 1 2 3 4 [Amato, Joseph. 1969. Mechanized Tracheotome [ permanent dead link ]. North Riverside, Illinois.
- ↑ [Howard, Adamson. 1985. Spring Operated Tracheotome Archived 2011-06-12 at the Wayback Machine . Margate, Florida.
- ↑ [Peterson, Leslie. 2006. Tracheal Tube/Tracheal Catheter Adaptor Cap Archived 2011-06-12 at the Wayback Machine . Castle Rock, CO.
- ↑ [Milhay, Alain. 1983. Tracheotomy Tube with Shield for Anesthesia Archived 2011-06-12 at the Wayback Machine . Amiens, France.
- 1 2 3 Tracheostomy, Balentine, Jerry. Medicine Net. Retrieved November 22, 2009.