Related Research Articles

A heart valve is a one-way valve that allows blood to flow in one direction through the chambers of the heart. Four valves are usually present in a mammalian heart and together they determine the pathway of blood flow through the heart. A heart valve opens or closes according to differential blood pressure on each side.

Tetralogy of Fallot (TOF), formerly known as Steno-Fallot tetralogy, is a congenital heart defect characterized by four specific cardiac defects. Classically, the four defects are:

dextro-Transposition of the great arteries is a potentially life-threatening birth defect in the large arteries of the heart. The primary arteries are transposed.

A congenital heart defect (CHD), also known as a congenital heart anomaly, congenital cardiovascular malformation, and congenital heart disease, is a defect in the structure of the heart or great vessels that is present at birth. A congenital heart defect is classed as a cardiovascular disease. Signs and symptoms depend on the specific type of defect. Symptoms can vary from none to life-threatening. When present, symptoms are variable and may include rapid breathing, bluish skin (cyanosis), poor weight gain, and feeling tired. CHD does not cause chest pain. Most congenital heart defects are not associated with other diseases. A complication of CHD is heart failure.
The Rastelli procedure is an open heart surgical procedure developed by Italian physician and cardiac surgery researcher, Giancarlo Rastelli, in 1967 at the Mayo Clinic, and involves using a pulmonary or aortic homograft conduit to relieve pulmonary obstruction in double outlet right ventricle with pulmonary stenosis.
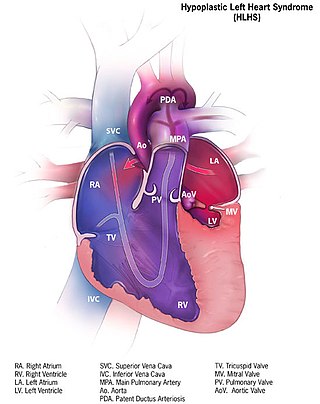
Hypoplastic left heart syndrome (HLHS) is a rare congenital heart defect in which the left side of the heart is severely underdeveloped and incapable of supporting the systemic circulation. It is estimated to account for 2-3% of all congenital heart disease. Early signs and symptoms include poor feeding, cyanosis, and diminished pulse in the extremities. The etiology is believed to be multifactorial resulting from a combination of genetic mutations and defects resulting in altered blood flow in the heart. Several structures can be affected including the left ventricle, aorta, aortic valve, or mitral valve all resulting in decreased systemic blood flow.
A transthoracic echocardiogram (TTE) is the most common type of echocardiogram, which is a still or moving image of the internal parts of the heart using ultrasound. In this case, the probe is placed on the chest or abdomen of the subject to get various views of the heart. It is used as a non-invasive assessment of the overall health of the heart, including a patient's heart valves and degree of heart muscle contraction. The images are displayed on a monitor for real-time viewing and then recorded.

Pulmonary atresia is a congenital malformation of the pulmonary valve in which the valve orifice fails to develop. The valve is completely closed thereby obstructing the outflow of blood from the heart to the lungs. The pulmonary valve is located on the right side of the heart between the right ventricle and pulmonary artery. In a normal functioning heart, the opening to the pulmonary valve has three flaps that open and close.

The Norwood procedure is the first of three surgeries intended to create a new functional systemic circuit in patients with hypoplastic left heart syndrome and other complex heart defects with single ventricle physiology. The first successful Norwood procedure involving the use of a cardiopulmonary bypass was reported by Dr. William Imon Norwood, Jr. and colleagues in 1981.
A right-to-left shunt is a cardiac shunt which allows blood to flow from the right heart to the left heart. This terminology is used both for the abnormal state in humans and for normal physiological shunts in reptiles.

Arterial switch operation (ASO) or arterial switch, is an open heart surgical procedure used to correct dextro-transposition of the great arteries (d-TGA).

A double inlet left ventricle (DILV) or "single ventricle", is a congenital heart defect appearing in 5 in 100,000 newborns, where both the left atrium and the right atrium feed into the left ventricle. The right ventricle is hypoplastic or does not exist.
Hypoplastic right heart syndrome is a congenital heart defect in which the structures on the right side of the heart, particularly the right ventricle, are underdeveloped. This defect causes inadequate blood flow to the lungs, and thus a cyanotic infant.

A ventricular outflow tract obstruction is a heart condition in which either the right or left ventricular outflow tract is blocked or obstructed. These obstructions represent a spectrum of disorders. Majority of these cases are congenital, but some are acquired throughout life.

Apicoaortic Conduit (AAC), also known as Aortic Valve Bypass (AVB), is a cardiothoracic surgical procedure that alleviates symptoms caused by blood flow obstruction from the left ventricle of the heart. Left ventricular outflow tract obstruction (LVOTO) is caused by narrowing of the aortic valve (aortic stenosis) and other valve disorders. AAC, or AVB, relieves the obstruction to blood flow by adding a bioprosthetic valve to the circulatory system to decrease the load on the aortic valve. When an apicoaortic conduit is implanted, blood continues to flow from the heart through the aortic valve. In addition, blood flow bypasses the native valve and exits the heart through the implanted valved conduit. The procedure is effective at relieving excessive pressure gradient across the natural valve. High pressure gradient across the aortic valve can be congenital or acquired. A reduction in pressure gradient results in relief of symptoms.
Fetal aortic stenosis is a disorder that occurs when the fetus’ aortic valve does not fully open during development. The aortic valve is a one way valve that is located between the left ventricle and the aorta, keeping blood from leaking back into the ventricle. It has three leaflets that separate when the ventricle contracts to allow blood to move from the ventricle to the aorta. These leaflets come together when the ventricle relaxes.
The Damus–Kaye–Stansel (DKS) procedure is a cardiovascular surgical procedure used as part of the repair of some congenital heart defects. This procedure joins the pulmonary artery and the aorta in situations where the systemic circulation is obstructed. It is commonly used when a patient has the combination of a small left ventricle and a transposition of the great arteries (TGA); in this case, the procedure allows blood to flow from the left ventricle to the aorta.
The LeCompte maneuver is a technique used in open heart surgery, primarily on infants and children. The maneuver entails cutting the main pulmonary artery and moving it anterior to the aorta before reattaching the pulmonary artery during the following reconstruction of the great vessels. It allows the surgeon to reconstruct the right ventricular outflow tract without needing to connect the proximal and distal sections with a graft. It also enables the surgeon to avoid compressing the coronary arteries and relieves compression of the bronchi in cases where the pulmonary artery is severely dilated or aneurysmal. If both pulmonary arteries are not mobilized adequately, they can become stretched, leading to pulmonic stenosis.

Pulmonary atresia with ventricular septal defect is a rare birth defect characterized by pulmonary valve atresia occurring alongside a defect on the right ventricular outflow tract.
References
- 1 2 3 Myers, Patrick; Sologashvili, Tornike; Wacker, Julie; Vallée, Jean-Paul; Beghetti, Maurice; Prêtre, René (9 December 2016). "Yasui procedure". Multimedia Manual of Cardio-Thoracic Surgery. 2016. doi:10.1510/mmcts.2016.005. ISSN 1813-9175. PMID 28195688.
- 1 2 Kanter, Kirk R.; Kirshbom, Paul M.; Kogon, Brian E. (June 2012). "Biventricular repair with the Yasui operation (Norwood/Rastelli) for systemic outflow tract obstruction with two adequate ventricles". The Annals of Thoracic Surgery. 93 (6): 1999–2005, discussion 2005–2006. doi: 10.1016/j.athoracsur.2012.02.050 . ISSN 1552-6259. PMID 22520828.
- ↑ Yasui, H.; Kado, H.; Nakano, E.; Yonenaga, K.; Mitani, A.; Tomita, Y.; Iwao, H.; Yoshii, K.; Mizoguchi, Y. (April 1987). "Primary repair of interrupted aortic arch and severe aortic stenosis in neonates". The Journal of Thoracic and Cardiovascular Surgery. 93 (4): 539–545. doi: 10.1016/S0022-5223(19)36381-0 . ISSN 0022-5223. PMID 3561000.
- ↑ Tchervenkov, Christo I.; Jacobs, Jeffrey P.; Sharma, Kapil; Ungerleider, Ross M. (2005). "Interrupted aortic arch: surgical decision making". Seminars in Thoracic and Cardiovascular Surgery. Pediatric Cardiac Surgery Annual. 8: 92–102. doi:10.1053/j.pcsu.2005.01.023. ISSN 1092-9126. PMID 15818364.
- ↑ Mahle, William T.; Crisalli, Joseph; Coleman, Karlene; Campbell, Robert M.; Tam, Vincent K. H.; Vincent, Robert N.; Kanter, Kirk R. (August 2003). "Deletion of chromosome 22q11.2 and outcome in patients with pulmonary atresia and ventricular septal defect". The Annals of Thoracic Surgery. 76 (2): 567–571. doi: 10.1016/s0003-4975(03)00516-2 . ISSN 0003-4975. PMID 12902105.
- ↑ Takabayashi, Shin; Kado, Hideaki; Shiokawa, Yuichi; Fukae, Kouji; Nakano, Toshihide (September 2005). "Long-term outcome of left ventricular outflow tract after biventricular repair using Damus-Kaye-Stansel anastomosis for interrupted aortic arch and severe aortic stenosis". The Journal of Thoracic and Cardiovascular Surgery. 130 (3): 942–944. doi: 10.1016/j.jtcvs.2005.05.030 . ISSN 0022-5223. PMID 16153978.