It is not performed if Marfan syndrome, pulmonary valve disease, or immune problems like lupus are present.[3] Other contraindications include severe coronary artery disease and severe mitral valve disease.[3] Due to a higher chance of dysfunction of the autograft, it may not always be safe to perform in rheumatic valve disease, or if a dysplastic dilated aortic root is present.[6] Complications include endocarditis, degeneration of the valves, aortic dissection, haemorrhage and venous thromboembolism, among others.[1][2] It risks having a disease of two valves instead of one.[7]
The procedure requires technical expertise.[4] It can be performed using the traditional subcoronary method or more commonly the root replacement technique, which requires re-implanting the coronary arteries.[8][9]
After the operation, good blood pressure control prevents early dilatation of the new aortic root and allows the pulmonary autograft, now in the aortic position, to settle in its new environment.[10] It may need reoperating on at a later date.[7] Complications occur in 3 to 5% of cases, with early death rate almost negligible in very experienced centres.[3] 80% to 90% of cases survive 10 years.[3] As of 2014, the Ross procedure comprises less than 1% of all aortic valve replacements in North America.[1]
The procedure was first performed using the subcoronary method in 1967 by Donald Ross, for whom the procedure is named.[8][11] The root replacement method was introduced in the early 1970s.[8] It was continued and modified by others such as Magdi Yacoub, who used fresh valves from the explanted hearts of transplant recipients.[11]
Uses
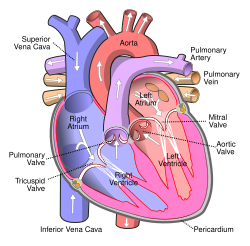
Diagram of the human heart
Several adaptations of the Ross procedure have evolved, but the principle is essentially the same; to replace a diseased aortic valve with the person's own pulmonary valve (autograft), and replace the person's own pulmonary valve with a pulmonary valve from a cadaver (homograft) or a stentless xenograft.[1][4] It is an alternative to a mechanical valve replacement, particularly in children and young adults.[7] It avoids the need for thinning the blood, has favourable blood flow dynamics and the valve grows as the person grows.[7]
The most common reason for performing the Ross procedure in children and young adults is for bicuspid aortic valve.[1]
Contra-indications
It is not performed in Marfan syndrome, if pulmonary valve disease, or if immune problems like lupus.[3] Other contraindications include severe coronary artery disease and severe mitral valve disease.[3] Due to a higher chance of dysfunction of the autograft, it may not always be safe to perform in rheumatic valve disease, or if a dysplastic dilated aortic root.[6]
Risks/complications
The procedure requires technical expertise, and risks converting a single-valve disease into double-valve disease.[4] It may need re-operating on at a later date.[7] Complications include endocarditis, degeneration of the valves, aortic dissection, haemorrhage and venous thromboembolism, among others.[1][2]
If the left sided outflow root needs to be enlarged to fit the pulmonary autograft, the procedure is called Ross-Konno.[3] An alternative to a pulmonary homograft is the stentless xenograft roots such as the Freestyle Porcine Aortic Root by Medtronic.[2][12] An external Dacron graft can be used to reinforce the pulmonary autograft.[2]
Recovery
After the operation, good blood pressure control prevents early dilatation of the new aortic root and allows the pulmonary autograft, now in the aortic position, to settle in its new environment.[10] Aftercare includes regular echocardiography and lifelong endocarditis prophylaxis.[1]
Epidemiology
Complications occur in 3% to 5% of cases with one to 3% chance of early death. The death rate is almost negligible in very experienced centres. 80% to 90% of cases survive 10 years, and 70% to 80% may live up to 20 years.[3] As of 2014, the Ross procedure comprises less than 1% of all aortic valve replacements in North America.[1]
History
Replacing a diseased aortic valve with an aortic valve from a cadaver was first performed by Donald Ross in England in June 1962, and shortly after in July 1962 by Brian Barratt-Boyes in Auckland, New Zealand.[11][13] In 1967 Ross took the normal pulmonary valve of a person with severe aortic valve disease, and placed it in the aortic position where the diseased aortic valve was removed.[11] To reconstruct the missing pulmonary outflow tract, a homograft stored and sterilised from a cadaver was used to replace the removed pulmonary valve.[11] In 1972, Ross introduced the technique using the root replacement method.[13] For 30 years he was almost the only surgeon performing the procedure, until it gained popularity.[11]Marian Ionescu in Leeds, in an attempt to seek other materials, unsuccessfully tried fascia lata from the person's own thigh to create a living valve.[11] He then tried successfully with cattle pericardium fixed with glutaraldehyde, and the procedure became widespread before then falling out of favour as they failed.[11] Then came pig valves (xenograft) before the 1980s trend for mechanical valves.[11] The Ross procedure was continued and modified by Magdi Yacoub, who used fresh valves from the explanted hearts of transplant recipients.[11]
Etymology
It has also been called the double-switch Ross procedure.[14]
The procedure was more popular in the 1990s and then declined in use over the subsequent 20 years.[16] Data relating to the procedure is held in the Ross registry.[17]
Other animals
The procedure has been carried out in pigs and sheep for the purpose of research.[18]
Footnotes
↑ With reference to valves, homograft refers to a valve from another human, xenograft usually from pig, and autograft as moving one valve from one place to another in the same person.[5]
↑ Bunce, Nicholas H.; Ray, Robin; Patel, Hitesh (2020). "30. Cardiology". In Feather, Adam; Randall, David; Waterhouse, Mona (eds.). Kumar and Clark's Clinical Medicine (10thed.). Elsevier. p.1102. ISBN978-0-7020-7870-5.
1 2 Morita, K.; Kurosawa, H. (April 2001). "[Indications for and clinical outcome of the Ross procedure: a review]". Nihon Geka Gakkai Zasshi. 102 (4): 330–336. ISSN0301-4894. PMID11344686.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.