Overview of the causes for and prevalence of obesity in Thailand
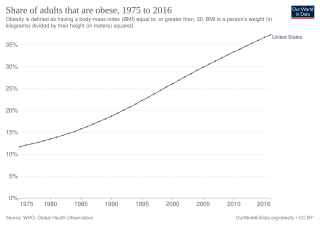
Share of adults that are obese, 1975 to 2016
Obesity in Thailand has been flagged as a major source of health concern,[1] with 32% of the population identifying as overweight and 9% obese.[2] With reference to 2016 data from the World Health Organization (WHO), Thailand has one of the highest incidence of overweight citizens in the South East Asian region, second to only Malaysia.[2] The Thai National Health Examination Surveys (NHES) found that obesity in Thailand more than doubled during the period 1991-2014.[3] This spike in obesity levels has been largely attributed to increased access to junk food,[4] and unhealthy switches from active to sedentary lifestyles.[5] These factors are closely linked to economic growth in the country.[5]
The internationally recognised method of measuring obesity is through the Body Mass Index (BMI). According to WHO, an overweight person has a BMI of ≥25. An obese person has a BMI of ≥30.[6] However, while the WHO standard has been used internationally, studies have shown that it may not be accurate for the classification of obesity in the Asian context due to different body fat percentages and body compositions.[7][8] Instead, an alternative standard should be used. As proposed by the International Association for the Study of Obesity and the International Obesity Task Force (IOTF) in 2000,[9] the Regional Office for the Western Pacific (WPRO) standard is more appropriate for Asian populations. According to WPRO, an overweight person has a BMI of ≥ 23. An obese person has a BMI of ≥25.
Obese male with a BMI of 52.8. Obesity levels have been on the rise in Thailand.
Prevalence of obesity in the Thai population
According to WHO, overweight and obesity levels in Thailand have been steadily increasing over the years. The percentage of overweight or obese adults increased from 8.6% in 1975 to 32.6% in 2016.[11]
Thai Adults
In 2004, a study involving 3,220 adults between the age 20 – 59 was carried out. The age-adjusted overweight and obesity levels were found to be 28.3% and 6.8%, respectively.[12]
Using the WPRO standard, results from the Thai Food Consumption Survey (TFCS) in 2005 showed that the combined prevalence of overweight and obesity in Thai adults aged 19 years and over exceeded 40%.[1] An estimated 17.1% of those surveyed fell under the classification of overweight (BMI 23.0 – 24.9), 19.0% categorised as class 1 obesity (BMI 25.0 – 29.9), and 4.8% as class 2 obesity (BMI ≥ 30.0).[1] It was also found that obesity had a larger impact on women than men, with combined obesity and overweight rates at 46.1% and 35.5%, respectively.[1] Obesity was more commonly found to occur in urban settings as compared to suburban areas.[1]
NHES is a nationwide survey which measures the health status of Thai citizens. As to date, 5 reports have been released over a period of 23 years. Namely in 1991, 1996, 2004,[13] 2009[14] and 2014. Results from the 2009 survey showed combined overweight and obesity levels to be at 41% for females and 28% for males. 5 years later, the 2014 survey showed the prevalence of overweight and obesity in females increased to 43% and rose to 33% in males.
In 2011, the WHO found that 32.6% of Thais were overweight,[11] ranking the country second heaviest in South East Asia, with higher obesity levels than more affluent nations including the Republic of Korea, Japan and Singapore.[15]
The Behavioural Risk Factor Surveillance System (BRFSS) was set up in 2005 to track the health status of Thais.[citation needed] It uses the WHO standard of BMI.[citation needed]
The prevalence of obesity in Thailand coincides with increased intake of sugary drinks. In 2010, it was reported that an average Thai consumed 93.9 litres of sweetened drinks on a yearly basis. This figure rose by 23.8% in 2015, to 115.6 litres.[16]
Children and adolescents
In 1992, a 5 year follow-up study involving primary and secondary schools of Hat Yai municipality, south Thailand was conducted. This study, involving 2,252 school children, tracked overweight prevalence from childhood to adolescence.[17] From the period 1992 to 1997, it was observed that 11.8% of children remained overweight.[17] It was concluded that overweight children face a much higher probability of being overweight as adults, and are at a higher risk of developing overweight related health diseases.[17]
Comparing results from NHES released in 1996 and a separate national survey conducted in 2001,[18][19] obesity levels in children aged 2 to 12 years experienced a rise. Obesity prevalence in preschool children (ages 2 to 5) increased from 5.8% in 1996 to 7.9% in 2001.[18] Children in the age group 6 to 12 years saw an increase in obesity rates from 5.8% to 6.7%.[19] Data also showed that obesity was a more prevalent problem amongst children living in urban areas, as compared to rural areas.[18]
In 2003, a nationwide survey was conducted by the National Health Foundation. It involved 47,389 grade 6 primary school children in urban settings.[20] From this, it was found that 16.7% of the children surveyed were either obese or overweight.[20]
In 2007, a school-based cross sectional study was conducted to determine the prevalence of obesity in Thai children in rural Ongkharak.[21] This study tracked the height and weight of 1,140 children between the ages 6 to 15. The results were based on the International Obesity Task Force standard and revealed the prevalence of overweight and obesity levels to be 12.8% and 9.4% respectively.[21]
In 2013, another study was conducted in Ongkharak, to establish the association of obesity with hypertension in school children. A total of 3,991 students with a mean age of 9.5 years were studied.[22] This study revealed that signs of hypertension were higher in obese and overweight children, as compared to children within the healthy weight range, at 49.5% and 26.5% versus 16.2% respectively.[22] Furthermore, it was found that prevalence of overweight and obesity levels were 13.8% and 15.5% respectively.[22] This is an increase from the previous study conducted in 2007.[21]
The Global Burden of Disease Study over the time period 1980 – 2013 showed that childhood obesity in developing countries increased from 8.1% to 12.9% for boys and from 8.4% to 13.4% in girls.[23]
Buddhist Monks
In 2006, a survey involving Buddhist monks and novices in Central Bangkok was carried out. The results showed that 35% of participants were at risk of developing obesity related health issues.[24]
In the following year, Priest Hospital released a report documenting the prevalence of obesity related health issues amongst monks. The study which consisted of 17,381 monks showed that 17.8% were diabetic, 17.1% had hypertension and 13.5% were found to have hyperlipidaemia.[25]
A study carried out by Chulalongkorn University in 2016 revealed obesity rates amongst monks to be at 48%. Approximately 42% of those surveyed displayed high cholesterol levels, 23% had high blood pressure and 10.4% were diabetic. In 2012 alone, healthcare costs borne by the Thai government amounted to $8.5 million (or 300 million baht).[26]
Most recently in 2017, the Ministry of Public Health (Thailand) surveyed monks from 200 temples, across 50 Bangkok districts. The study revealed high blood cholesterol and high blood sugar plaguing 60% and 50% of those surveyed, respectively.[27]
Obesity amongst monks has been attributed to lack of exercise and overnutrition from unhealthy food offered by devotees.[28] Following the Buddhist discipline, monks cannot reject alms given to them, which usually consists of food that are high in fat and sugar.[29][30] Furthermore, exercise is usually shunned by monks as it is seen as a form of egotism.[28]
Diabetes and cost of obesity
In a statement released by the Thai Ministry of Public Health, Non-communicable diseases (NCDs) were listed as the ‘No. 1 health issue’ in the country, ‘both in terms of number (of) casualties and burden of disease’.[31]Diabetes was also flagged as one of the major components of NCDs plaguing the Thai population.[31] Comparing data from NHES conducted in 2009 and 2014, the prevalence of diabetes increased from 6.9% to 8.9% (or an increase of about 300,000 citizens annually).[31] As of 2017, 8.3% of Thai adults were diabetic.[32]
Referencing the death register of the Bureau of Registration Administration, Ministry of Interior, it was found that between 2012-2015, the number of premature deaths caused by NCDs increased. In particular, it was found that deaths by diabetes increased from 13.2 to 17.8 per 100,000 people.[31]
A 2009 joint study between the Health Intervention and Technology Assessment Program (HITAP) of the Ministry of Public Health and Mahidol University showed that the cost of obesity on the Thai health system amounted to $404 million or 12 billion baht annually.[33] The research further revealed that direct health care cost for patients accounted for 46% (or $186 million) of total obesity costs. Indirect health care costs made up the remaining 54% (or $218 million), with opportunity costs related to premature deaths totalling $195 million and hospital related absenteeism totalling $23 million.[33]
Government responses
Over the years, the Thai government has launched a series of health campaigns in an attempt to reverse this increasing obesity trend in the country. From 2002 to 2017, campaigns aimed at encouraging healthy habits among Thais took up 92% of the yearly ThaiHealth expenditure.[34]
Studies have shown that childhood obesity tends to lead to adult obesity.[35] As a result, it has been suggested by academics that efforts to curb and prevent overweight and obesity should start in childhood.[36]
‘Foods for Children’
The strong presence of fast food advertising on Thai television has been identified as a major culprit in the development of unhealthy eating habits.[37][38][39] In 2007, in an attempt to reverse this, the Thai Food and Drug Administration (FDA) and Public Relations Department placed restrictions on food advertisements targeting children on prime-time television.[40] ‘Foods for Children’ related advertisements were only allowed screen time of 12 mins per hour. In addition, fast food toys were banned and all unhealthy products had to be labelled with ‘Eat Less, Exercise More”.[40]
Promoting regular exercise and physical activity
Efforts to encourage regular exercise and physical activity have been seen on the part of the Ministry of Public Health since 2009.[40] Such initiatives include setting up exercise corners in public areas within society. To further promote physical activity, bike lanes have been set up across the country.[41] This has positively impacted physical activity levels among Thai adults, which increased from 66.3% to 72.9% between 2012 and 2017.[42]
‘Thai People Have Flat Belly’
Launched in 2010, this campaigned for healthy food consumption and higher levels of exercise to reduce non-communicable diseases.[43] A similar approach was taken by the Royal College of Physicians of Thailand to launch ‘Network of Flatless Belly Thais’ to reduce intra-abdominal adiposity and metabolic syndrome for Thai citizens.[43]
‘Sweet Enough Network’
In 2010, 'Sweet Enough Network' was set up by the Ministry of Public Health’s Dental Health Division, to push for tighter regulations regarding sugary drinks in Thailand. This campaign advocated the banning of sugary drinks sold in educational institutions as well as added sugar found in follow-up milk powder for babies.[40] The Thai government responded by implementing a nationwide ban of added sugar in follow-up milk powder for babies.[40]
Sugar tax on sweetened drinks
In 2017, a sugar tax on sweetened beverages was implemented by the Thai National Legislative Council. This was seen as an attempt to curb heightened levels of overweight and obesity in the country.[44] Sweetened drinks are subjected to a 14% excise tax on the suggested selling price, along with an additional tax on its sugar content.[45] This sugar tax is projected to rise every 2 years, over a period of 6 years.[46] As a result of this, sugar consumption within the country decreased by 3% between the time period 2017 and 2018.[47]
Health Charter for Buddhist Monks
In 2017, the Health Charter for Buddhist was launched, in an attempt to promote healthy living and curb obesity levels amongst Thai monks. This was implemented with the aim of creating self-awareness on health issues that are in line with Buddhist values as well as educating the public about importance of healthy eating.[48]
↑ "BMI classification". World Health Organization. | access-date= 2014-2-15.
↑ Deurenberg, P; Deurenberg-Yap, M; Guricci, S (2002). "Asians are different from Caucasians and from each other in their body mass index/body fat percent relationship". Obes Rev. 3 (3): 141–6. doi:10.1046/j.1467-789x.2002.00065.x. PMID12164465.
↑ Low, S; Chin, MC; Ma, S; etal. (2009). "Rationale for redefining obesity in Asians". Ann Acad Med Singapore. 38: 66–74.
↑ World Health Organization, Regional Office for the Western Pacific (WPRO), International Association for the Study of Obesity, International Obesity Task Force. The Asia-Pacific Perspective: Redefining obesity and its treatment. Sydney: Health Communications Australia Pty Ltd; 2000.
↑ Aekplakorn, W.; Chaiyapong, Y.; Neal, B. (2004). "Prevalence and determinants of overweight and obesity in Thai adults: Results of the Second National Health Examination Survey". Journal of the Medical Association of Thailand. 87: 685–693.
↑ Cheong, W. S. 2014. "Overweight and Obesity in Asia." Underwriting Focus, no. December 2014 (2014). http://www.genre.com/knowledge/publications/ uwfocus14-2-cheong-en.html (accessed 30 July 2016).
1 2 3 Sanguansak R, Lakkana R: Prevalence of Overweight and Obesity Among School Children in Suburb Thailand Defined by the International Obesity Task Force standard. J Med Assoc Thai 2010, 93(2):S27–31.
1 2 3 Rerksuppaphol S, Rerksuppaphol L. Association of Obesity with the Prevalence of Hypertension in School Children from Central Thailand. J Res Health Sci. 2015; 15(1): 17-21.
↑ Bhumisawasdi, V; Takerngdej, S; Jenchitr, W (2008). "The sustained and holistic health care program for the priests Commemoration of His Majesty the King's 60 years Accession to the Throne (first phase: February to June 2006)". J Med Assoc Thail. 91 (Suppl 1): S1–S12.
↑ Kuramasuwan, Bhuwadol; Howteerakul, Nopporn; Suwannapong, Nawarat; Rawdaree, Petch (2013-03-01). "Diabetes, impaired fasting glucose, daily life activities, food and beverage consumption among Buddhist monks in Chanthaburi Province, Thailand". International Journal of Diabetes in Developing Countries. 33 (1): 23–28. doi:10.1007/s13410-012-0094-y. ISSN1998-3832.
↑ Wang, Youfa; Lobstein, Tim (2006). "Worldwide trends in childhood overweight and obesity". International Journal of Pediatric Obesity. 1 (1): 11–25. doi:10.1080/17477160600586747. ISSN1747-7174.
↑ Saowaphak N. Master of Mass Communications dissertation.Thurakit Banthit University; Bangkok, Thailand: 1995. The influence of marketing on the consumption of fast foods among young people in Bangkok.
↑ Saeiew, Khanitta. "Health Charter for Buddhist Monks, established healthy monks, temples and happy communities in 10 years". National Health Commission Office (Thailand). Retrieved 16 May 2019.
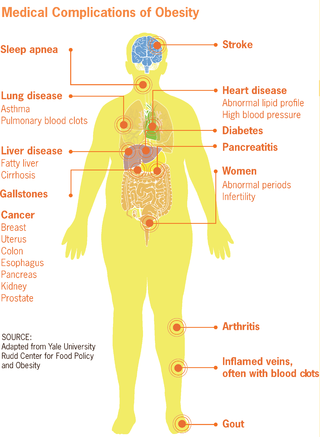
Obesity is a medical condition, sometimes considered a disease, in which excess body fat has accumulated to such an extent that it can potentially have negative affects on health. People are classified as obese when their body mass index (BMI)—a person's weight divided by the square of the person's height—is over 30 kg/m2; the range 25–30 kg/m2 is defined as overweight. Some East Asian countries use lower values to calculate obesity. Obesity is a major cause of disability and is correlated with various diseases and conditions, particularly cardiovascular diseases, type 2 diabetes, obstructive sleep apnea, certain types of cancer, and osteoarthritis.
Human body weight is a person's mass or weight.
Diseases of affluence, previously called diseases of rich people, is a term sometimes given to selected diseases and other health conditions which are commonly thought to be a result of increasing wealth in a society. Also referred to as the "Western disease" paradigm, these diseases are in contrast to so-called "diseases of poverty", which largely result from and contribute to human impoverishment. These diseases of affluence have vastly increased in prevalence since the end of World War II.
Childhood obesity is a condition where excess body fat negatively affects a child's health or well-being. As methods to determine body fat directly are difficult, the diagnosis of obesity is often based on BMI. Due to the rising prevalence of obesity in children and its many adverse health effects it is being recognized as a serious public health concern. The term 'overweight' rather than 'obese' is often used when discussing childhood obesity, as it is less stigmatizing, although the term 'overweight' can also refer to a different BMI category. The prevalence of childhood obesity is known to differ by sex and gender.
Obesity in Mexico is a relatively recent phenomenon, having been widespread since the 1980s with the introduction of ultra-processed food into much of the Mexican food market. Prior to that, dietary issues were limited to under and malnutrition, which is still a problem in various parts of the country. Following trends already ongoing in other parts of the world, Mexicans have been foregoing the traditional Mexican diet high in whole grains, fruits, legumes and vegetables in favor of a diet with more animal products and ultra-processed foods. It has seen dietary energy intake and rates of overweight and obese people rise with seven out of ten at least overweight and a third clinically obese.
Obesity is common in the United States and is a major health issue associated with numerous diseases, specifically an increased risk of certain types of cancer, coronary artery disease, type 2 diabetes, stroke, and cardiovascular disease, as well as significant increases in early mortality and economic costs.
Obesity is a risk factor for many chronic physical and mental illnesses.
Obesity has been observed throughout human history. Many early depictions of the human form in art and sculpture appear obese. However, it was not until the 20th century that obesity became common — so much so that, in 1997, the World Health Organization (WHO) formally recognized obesity as a global epidemic and estimated that the worldwide prevalence of obesity has nearly tripled since 1975. Obesity is defined as having a body mass index (BMI) greater than or equal to 30 kg/m2, and in June 2013 the American Medical Association classified it as a disease.
Obesity in Canada is a growing health concern, which is "expected to surpass smoking as the leading cause of preventable morbidity and mortality" and represents a burden of Can$3.96 (US$3.04/€2.75) billion on the Canadian economy each year."
Diet plays an important role in the genesis of obesity. Personal choices, food advertising, social customs and cultural influences, as well as food availability and pricing all play a role in determining what and how much an individual eats.
Obesity in the United Kingdom is a significant contemporary health concern, with authorities stating that it is one of the leading preventable causes of death. In February 2016, former Health Secretary Jeremy Hunt described rising rates of childhood obesity as a "national emergency". The National Childhood Measurement Programme, which measures obesity prevalence among school-age pupils in reception class and year 6, found obesity levels rocketed in both years groups by more than 4 percentage points between 2019–20 and 2020–21, the highest rise since the programme began. Among reception-aged children, those aged four and five, the rates of obesity rose from 9.9% in 2019–20 to 14.4% in 2020–21. By the time they are aged 10 or 11, more than a quarter are obese. In just 12 months, the rate is up from 21% in 2019–20 to 25.5% in 2020–21.
According to 2007 statistics from the World Health Organization (WHO), Australia has the third-highest prevalence of overweight adults in the English-speaking world. Obesity in Australia is an "epidemic" with "increasing frequency." The Medical Journal of Australia found that obesity in Australia more than doubled in the two decades preceding 2003, and the unprecedented rise in obesity has been compared to the same health crisis in America. The rise in obesity has been attributed to poor eating habits in the country closely related to the availability of fast food since the 1970s, sedentary lifestyles and a decrease in the labour workforce.
Pacific island nations and associated states make up the top seven on a 2007 list of heaviest countries, and eight of the top ten. In all these cases, more than 70% of citizens aged 15 and over are obese. A mitigating argument is that the BMI measures used to appraise obesity in Caucasian bodies may need to be adjusted for appraising obesity in Polynesian bodies, which typically have larger bone and muscle mass than Caucasian bodies; however, this would not account for the drastically higher rates of cardiovascular disease and type 2 diabetes among these same islanders.
Obesity in the Middle East and North Africa is a notable health issue. Out of the fifteen fattest nations in the world as of 2014, 5 were located in the Middle East and North Africa region.
A person's waist-to-height ratio (WHtR), occasionally written WtHR or called waist-to-stature ratio (WSR), is defined as their waist circumference divided by their height, both measured in the same units. It is used as a predictor of obesity-related cardiovascular disease. The WHtR is a measure of the distribution of body fat. Higher values of WHtR indicate higher risk of obesity-related cardiovascular diseases; it is correlated with abdominal obesity.
Obesity in Pakistan is a health issue that has effected concern only in the past few years. Urbanisation, fast food, changing lifestyles and the fact that Traditional Pakistani Cuisine tends to be high in fat and sugar are among the root causes contributing to obesity in the country. Pakistan is ranked 165 in terms of its overweight population, with 22.2% of individuals over the age of 15 crossing the threshold of obesity. This ratio roughly corresponds with other studies, which state one-in-four Pakistani adults as being overweight. In Pakistan, the problem of excess weight is quite high among adults.
A sweetened beverage is any beverage with added sugar. It has been described as "liquid candy". Consumption of sweetened beverages has been linked to weight gain, obesity, and associated health risks. According to the CDC, consumption of sweetened beverages is also associated with unhealthy behaviors like smoking, not getting enough sleep and exercise, and eating fast food often and not enough fruits regularly.
Childhood obesity is defined as a body mass index (BMI) at or above the 96th percentile for children of the same age and sex. It can cause a variety of health problems, including high blood pressure, high cholesterol, heart disease, diabetes, breathing problems, sleeping problems, and joint problems later in life. Children who are obese are at a greater risk for social and psychological problems as well, such as peer victimization, increased levels of aggression, and low self-esteem. Many environmental and social factors have been shown to correlate with childhood obesity, and researchers are attempting to use this knowledge to help prevent and treat the condition. When implemented early, certain forms of behavioral and psychological treatment can help children regain and/or maintain a healthy weight.
Within the Pacific, Tonga is recognised to have some of the highest overall health standards, implementing a combination of preventative and immediate strategies to curb rates of communicable disease, child mortality and overall life expectancy. The Tongan government aims to continue such levels of health through achieving their Millennium Development Goals (MDG) detailing their focus on improving their healthcare system within the areas of maternal and infant health as well as improve access to immunisation, safe water and sanitation.
According to the World Health Organization (2015), the "worldwide population of overweight and obese adults increased between 1980 and 2013 from 30 percent to 38 percent in women, and 29 percent to 37 percent in men". The prevalence of obesity continues to rise in all age groups in this developing country.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.