For most people, the first symptoms result from atheroma progression within the heart arteries, most commonly resulting in a heart attack and ensuing debility. The heart arteries are difficult to track because they are small (from about 5mm down to microscopic), they are hidden deep within the chest and they never stop moving. Additionally, all mass-applied clinical strategies focus on both minimal cost and the overall safety of the procedure. Therefore, existing diagnostic strategies for detecting atheroma and tracking response to treatment have been extremely limited. The methods most commonly relied upon, patient symptoms and cardiac stress testing, do not detect any symptoms of the problem until atheromatous disease is very advanced because arteries enlarge, not constrict, in response to increasing atheroma.[6] It is plaque ruptures, producing debris and clots which obstruct blood flow downstream, sometimes also locally (as seen on angiograms), which reduce/stop blood flow. Yet these events occur suddenly and are not revealed in advance by either stress tests[7] or angiograms.[8][9]
Mechanism
The healthy epicardial coronary artery consists of three layers, the tunica intima, media, and adventitia.[10][11] Atheroma and changes in the artery wall usually result in small aneurysms (enlargements) just large enough to compensate for the extra wall thickness with no change in the lumen diameter. However, eventually, typically as a result of rupture of vulnerable plaques and clots within the lumen over the plaque, stenosis (narrowing) of the vessel develops in some areas. Less frequently, the artery enlarges so much that a gross aneurysmal enlargement of the artery results. All three results are often observed, at different locations, within the same individual.[12][13]
Stenosis and closure
Over time, atheromata usually progress in size and thickness and induce the surrounding muscular central region (the media) of the artery to stretch out, which is termed remodeling. Typically, remodeling occurs just enough to compensate for the atheroma's size such that the calibre of the artery opening (lumen) remains unchanged, until about 50% of the artery wall cross-sectional area consists of atheromatous tissue.[6]
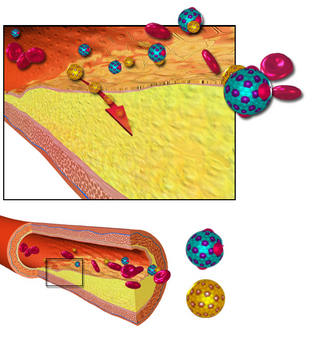
Narrowed arterial blood vessel blocked with an atheroma (artist's conception).
If the muscular wall enlargement eventually fails to keep up with the enlargement of the atheroma volume, or a clot forms and organizes over the plaque, then the lumen of the artery becomes narrowed as a result of repeated ruptures, clots and fibrosis over the tissues separating the atheroma from the blood stream. This narrowing becomes more common after decades of living, increasingly more common after people are in their 30s to 40s.[citation needed]
The endothelium (the cell monolayer on the inside of the vessel) and covering tissue, termed fibrous cap, separate atheroma from the blood in the lumen. If a rupture (see vulnerable plaque) of the endothelium and fibrous cap occurs, then both a shower of debris from the plaque (debris larger than 5 micrometres are too large to pass through capillaries) combined with a platelet and clotting response (an injury/repair response to both the debris and at the rupture site) begins within fractions of a second, eventually resulting in narrowing or sometimes closure of the lumen. Eventually downstream tissue damage occurs due to closure or obstruction of downstream microvessels and/or closure of the lumen at the rupture, both resulting in loss of blood flow to downstream tissues. This is the principal mechanism of myocardial infarction, stroke or other related cardiovascular disease problems.[citation needed]
While clots at the rupture site typically shrink in volume over time, some of the clot may become organized into fibrotic tissue resulting in narrowing of the artery lumen; the narrowings sometimes seen on angiography examinations, if severe enough. Since angiography methods can only reveal larger lumens, typically larger than 200 micrometres, angiography after a cardiovascular event commonly does not reveal what happened.[citation needed]
Artery enlargement
If the muscular wall enlargement is overdone over time, then a gross enlargement of the artery results, usually over decades of living. This is a less common outcome. Atheroma within aneurysmal enlargement (vessel bulging) can also rupture and shower debris of atheroma and clot downstream. If the arterial enlargement continues to 2 to 3 times the usual diameter, the walls often become weak enough that with just the stress of the pulse, a loss of wall integrity may occur leading to sudden hemorrhage (bleeding), major symptoms and debility; often rapid death. The main stimulus for aneurysm formation is pressure atrophy of the structural support of the muscle layers. The main structural proteins are collagen and elastin. This causes thinning and the wall balloons allowing gross enlargement to occur, as is common in the abdominal region of the aorta.[citation needed]
After they accumulate large amounts of cytoplasmic membranes (with associated high cholesterol content) they are called foam cells. When foam cells die, their contents are released, which attracts more macrophages and creates an extracellular lipid core near the centre to inner surface of each atherosclerotic plaque. [citation needed]
Conversely, the outer, older portions of the plaque become more calcified, less metabolically active and more physically stiff over time.[citation needed]
Veins do not develop atheromata, because they are not subjected to the same haemodynamic pressure that arteries are,[14] unless surgically moved to function as an artery, as in bypass surgery.
Diagnosis
Illustration comparing a normal blood vessel and partially blocked vessel due to atherosclerotic plaque. Notice the enlargement & absence of much luminal narrowing.
Because artery walls enlarge at locations with atheroma,[6] detecting atheroma before death and autopsy has long been problematic at best. Most methods have focused on the openings of arteries; while these methods are highly relevant, they totally miss the atheroma within the arterial lumen.[citation needed]
Historically, arterial wall fixation, staining and thin section has been the gold standard for detection and description of atheroma, after death and autopsy. With special stains and examination, micro calcifications[15] can be detected, typically within smooth muscle cells of the arterial media near the fatty streaks within a year or two of fatty streaks forming.
Interventional and non-interventional methods to detect atherosclerosis, specifically vulnerable plaque (non-occlusive or soft plaque), are widely used in research and clinical practice today.[citation needed]
Intravascular ultrasound is the current most sensitive method detecting and measuring more advanced atheroma within living individuals, but has had limited applications due to cost and body invasiveness.[17][18]
CT scans using state of the art higher resolution spiral, or the higher speed EBT, machines have been the most effective method for detecting calcification present in plaque. However, the atheroma have to be advanced enough to have relatively large areas of calcification within them to create large enough regions of ~130 Hounsfield units which a CT scanner's software can recognize as distinct from the other surrounding tissues. Typically, such regions start occurring within the heart arteries about 2–3 decades after atheroma start developing. The presence of smaller, spotty plaques may actually be more dangerous for progressing to acute myocardial infarction.[19]
Arterial ultrasound, especially of the carotid arteries, with measurement of the thickness of the artery wall, offers a way to partially track the disease progression. As of 2006, the thickness, commonly referred to as IMT for intimal-medial thickness, is not measured clinically though it has been used by some researchers since the mid-1990s to track changes in arterial walls. Traditionally, clinical carotid ultrasounds have only estimated the degree of blood lumen restriction, stenosis, a result of very advanced disease. The National Institute of Health did a five-year $5 million study, headed by medical researcherKenneth Ouriel, to study intravascular ultrasound techniques regarding atherosclerotic plaque.[citation needed] More progressive clinicians have begun using IMT measurement as a way to quantify and track disease progression or stability within individual patients.[citation needed]
Angiography, since the 1960s, has been the traditional way of evaluating for atheroma. However, angiography is only motion or still images of dye mixed with the blood within the arterial lumen and never show atheroma; the wall of arteries, including atheroma within the arterial wall remain invisible. The limited exception to this rule is that with very advanced atheroma, with extensive calcification within the wall, a halo-like ring of radiodensity can be seen in most older humans, especially when arterial lumens are visualized end-on. On cine-floro, cardiologists and radiologists typically look for these calcification shadows to recognize arteries before they inject any contrast agent during angiograms.[citation needed]
This section needs more reliable medical references for verification or relies too heavily on primary sources, specifically: Out of ten points, only 4 are referenced, and among those only one is a primary, peer-reviewed reference. Without the medical refs, it's unclear how reliable each advised approach is pertaining to treating the disease, even if it is a good general advice. Please review the contents of the section and add the appropriate references if you can. Unsourced or poorly sourced material may be challenged and removed. Find sources:"Atheroma"–news·newspapers·books·scholar·JSTOR(October 2019)
Many approaches have been promoted[by whom?] as methods to reduce or reverse[21] atheroma progression:[citation needed]
eating a diet of raw fruits, vegetables, nuts, beans, berries, and grains;[21][22]
consuming foods containing omega−3 fatty acids such as fish, fish-derived supplements, as well as flax seed oil, borage oil, and other non-animal-based oils;
maintaining normal, or healthy, blood pressure levels;
aspirin supplement
mouse studies indicated that subcutaneous administration of oligosaccharide 2-hydroxypropyl-β-cyclodextrin (2HPβCD) can solubilize cholesterol, removing it from plaques.[23] However, later work concluded that "treatment with 2HPβCD is ineffective in inducing atherosclerosis regression".[24]
History of research
In developed countries, with improved public health, infection control and increasing life spans, atheroma processes have become an increasingly important problem and burden for society. Atheromata continue to be the primary underlying basis for disability and death, despite a trend for gradual improvement since the early 1960s (adjusted for patient age). Thus, increasing efforts towards better understanding, treating and preventing the problem are continuing to evolve.[citation needed]
According to United States data, 2004, for about 65% of men and 47% of women, the first symptom of cardiovascular disease is myocardial infarction (heart attack) or sudden death (death within one hour of symptom onset).[citation needed]
A significant proportion of artery flow-disrupting events occur at locations with less than 50% lumenal narrowing. Cardiac stress testing, traditionally the most commonly performed non-invasive testing method for blood flow limitations, generally only detects lumen narrowing greater than about 75%, although some physicians advocate nuclear stress tests that can sometimes detect as little as 50%.[citation needed]
The sudden nature of the complications of pre-existing atheroma, vulnerable plaque (non-occlusive or soft plaque), have led, since the 1950s, to the development of intensive care units and complex medical and surgical interventions. Angiography and later cardiac stress testing was begun to either visualize or indirectly detect stenosis. Next came bypass surgery, to plumb transplanted veins, sometimes arteries, around the stenoses and more recently angioplasty, now including stents, most recently drug coated stents, to stretch the stenoses more open.[citation needed]
Yet despite these medical advances, with success in reducing the symptoms of angina and reduced blood flow, atheroma rupture events remain the major problem and still sometimes result in sudden disability and death despite even the most rapid, massive and skilled medical and surgical intervention available anywhere today. According to some clinical trials, bypass surgery and angioplasty procedures have had at best a minimal effect, if any, on improving overall survival. Typically mortality of bypass operations is between 1 and 4%, of angioplasty between 1 and 1.5%.[citation needed]
Additionally, these vascular interventions are often done only after an individual is symptomatic, often already partially disabled, as a result of the disease. It is also clear that both angioplasty and bypass interventions do not prevent future heart attack.[citation needed]
The older methods for understanding atheroma, dating to before World War II, relied on autopsy data. Autopsy data has long shown initiation of fatty streaks in later childhood with slow asymptomatic progression over decades.[6]
One way to see atheroma is the very invasive and costly IVUS ultrasound technology; it gives us the precise volume of the inside intima plus the central media layers of about 25mm (1in) of artery length. Unfortunately, it gives no information about the structural strength of the artery. Angiography does not visualize atheroma; it only makes the blood flow within blood vessels visible. Alternative methods that are non or less physically invasive and less expensive per individual test have been used and are continuing to be developed, such as those using computed tomography (CT; led by the electron beam tomography form, given its greater speed) and magnetic resonance imaging (MRI). The most promising since the early 1990s has been EBT, detecting calcification within the atheroma before most individuals start having clinically recognized symptoms and debility. Statin therapy (to lower cholesterol) does not slow the speed of calcification as determined by CT scan. MRI coronary vessel wall imaging, although currently limited to research studies, has demonstrated the ability to detect vessel wall thickening in asymptomatic high risk individuals.[25] As a non-invasive, ionising radiation free technique, MRI based techniques could have future uses in monitoring disease progression and regression. Most visualization techniques are used in research, they are not widely available to most patients, have significant technical limitations, have not been widely accepted and generally are not covered by medical insurance carriers.[citation needed]
From human clinical trials, it has become increasingly evident that a more effective focus of treatment is slowing, stopping and even partially reversing the atheroma growth process.[22] There are several prospective epidemiologic studies including the Atherosclerosis Risk in Communities (ARIC) Study and the Cardiovascular Health Study (CHS), which have supported a direct correlation of CarotidIntima-media thickness (CIMT) with myocardial infarction and stroke risk in patients without cardiovascular disease history. The ARIC Study was conducted in 15,792 individuals between 5 and 65 years of age in four different regions of the US between 1987 and 1989. The baseline CIMT was measured and measurements were repeated at 4- to 7-year intervals by carotid B mode ultrasonography in this study. An increase in CIMT was correlated with an increased risk for CAD. The CHS was initiated in 1988, and the relationship of CIMT with risk of myocardial infarction and stroke was investigated in 4,476 subjects 65 years of age and below. At the end of approximately six years of follow-up, CIMT measurements were correlated with cardiovascular events.[citation needed]
Paroi artérielle et Risque Cardiovasculaire in Asia Africa/Middle East and Latin America (PARC-AALA) is another important large-scale study, in which 79 centres from countries in Asia, Africa, the Middle East, and Latin America participated, and the distribution of CIMT according to different ethnic groups and its association with the Framingham cardiovascular score was investigated. Multi-linear regression analysis revealed that an increased Framingham cardiovascular score was associated with CIMT, and carotid plaque independent of geographic differences.[citation needed]
Cahn et al. prospectively followed-up 152 patients with coronary artery disease for 6–11 months by carotid artery ultrasonography and noted 22 vascular events (myocardial infarction, transient ischemic attack, stroke, and coronary angioplasty) within this time period. They concluded that carotid atherosclerosis measured by this non-interventional method has prognostic significance in coronary artery patients.[citation needed]
In the Rotterdam Study, Bots et al. followed 7,983 patients >55 years of age for a mean period of 4.6 years, and reported 194 incident myocardial infarctions within this period. CIMT was significantly higher in the myocardial infarction group compared to the other group. Demircan et al. found that the CIMT of patients with acute coronary syndrome were significantly increased compared to patients with stable angina pectoris.[citation needed]
It has been reported in another study that a maximal CIMT value of 0.956mm had 85.7% sensitivity and 85.1% specificity to predict angiographic CAD. The study group consisted of patients admitted to the cardiology outpatient clinic with symptoms of stable angina pectoris. The study showed CIMT was higher in patients with significant CAD than in patients with non-critical coronary lesions. Regression analysis revealed that thickening of the mean intima-media complex more than 1.0 was predictive of significant CAD our patients. There was incremental significant increase in CIMT with the number coronary vessel involved. In accordance with the literature, it was found that CIMT was significantly higher in the presence of CAD. Furthermore, CIMT was increased as the number of involved vessels increased and the highest CIMT values were noted in patients with left main coronary involvement. However, human clinical trials have been slow to provide clinical & medical evidence, partly because the asymptomatic nature of atheromata make them especially difficult to study. Promising results are found using carotid intima-media thickness scanning (CIMT can be measured by B-mode ultrasonography), B-vitamins that reduce a protein corrosive, homocysteine and that reduce neck carotid artery plaque volume and thickness, and stroke, even in late-stage disease.[citation needed]
Additionally, understanding what drives atheroma development is complex with multiple factors involved, only some of which, such as lipoproteins, more importantly lipoprotein subclass analysis, blood sugar levels and hypertension are best known and researched. More recently, some of the complex immune system patterns that promote, or inhibit, the inherent inflammatory macrophage triggering processes involved in atheroma progression are slowly being better elucidated in animal models of atherosclerosis.[citation needed]
Angina, also known as angina pectoris, is chest pain or pressure, usually caused by insufficient blood flow to the heart muscle (myocardium). It is most commonly a symptom of coronary artery disease.
Atherosclerosis is a pattern of the disease arteriosclerosis, characterized by development of abnormalities called lesions in walls of arteries. These lesions may lead to narrowing of the arteries' walls due to buildup of atheromatous plaques. At onset there are usually no symptoms, but if they develop, symptoms generally begin around middle age. In severe cases, it can result in coronary artery disease, stroke, peripheral artery disease, or kidney disorders, depending on which body parts(s) the affected arteries are located in the body.
Arteriosclerosis is a vascular disorder characterized by abnormal thickening, hardening, and loss of elasticity of the walls of arteries; this process gradually restricts the blood flow to one's organs and tissues and can lead to severe health risks brought on by atherosclerosis, which is a specific form of arteriosclerosis caused by the buildup of fatty plaques, cholesterol, and some other substances in and on the artery walls.
A coronary catheterization is a minimally invasive procedure to access the coronary circulation and blood filled chambers of the heart using a catheter. It is performed for both diagnostic and interventional (treatment) purposes.
Restenosis is the recurrence of stenosis, a narrowing of a blood vessel, leading to restricted blood flow. Restenosis usually pertains to an artery or other large blood vessel that has become narrowed, received treatment to clear the blockage and subsequently become renarrowed. This is usually restenosis of an artery, or other blood vessel, or possibly a vessel within an organ.
A cardiac stress test is a cardiological test that measures the heart's ability to respond to external stress in a controlled clinical environment. The stress response is induced by exercise, intravenous pharmacological (drug) stimulation, or in some cases, a combination of both.
Coronary thrombosis is defined as the formation of a blood clot inside a blood vessel of the heart. This blood clot may then restrict blood flow within the heart, leading to heart tissue damage, or a myocardial infarction, also known as a heart attack.
Intravascular ultrasound (IVUS) or intravascular echocardiography is a medical imaging methodology using a specially designed catheter with a miniaturized ultrasound probe attached to the distal end of the catheter. The proximal end of the catheter is attached to computerized ultrasound equipment. It allows the application of ultrasound technology, such as piezoelectric transducer or CMUT, to see from inside blood vessels out through the surrounding blood column, visualizing the endothelium of blood vessels.
A vulnerable plaque is a kind of atheromatous plaque – a collection of white blood cells and lipids in the wall of an artery – that is particularly unstable and prone to produce sudden major problems such as a heart attack or stroke.
Carotid artery stenosis is a narrowing or constriction of any part of the carotid arteries, usually caused by atherosclerosis.
Fractional flow reserve (FFR) is a diagnostic technique used in coronary catheterization. FFR measures pressure differences across a coronary artery stenosis to determine the likelihood that the stenosis impedes oxygen delivery to the heart muscle.
Intima–media thickness (IMT), also called intimal medial thickness, is a measurement of the thickness of tunica intima and tunica media, the innermost two layers of the wall of an artery. The measurement is usually made by external ultrasound and occasionally by internal, invasive ultrasound catheters. Measurements of the total wall thickness of blood vessels can also be done using other imaging modalities.
A coronary stent is a tube-shaped device placed in the coronary arteries that supply blood to the heart, to keep the arteries open in the treatment of coronary heart disease. It is used in a procedure called percutaneous coronary intervention (PCI). Coronary stents are now used in more than 90% of PCI procedures. Stents reduce angina and have been shown to improve survival and decrease adverse events in an acute myocardial infarction.
Coronary artery aneurysm is an abnormal dilatation of part of the coronary artery. This rare disorder occurs in about 0.3–4.9% of patients who undergo coronary angiography.
Coronary ischemia, myocardial ischemia, or cardiac ischemia, is a medical term for a reduced blood flow in the coronary circulation through the coronary arteries. Coronary ischemia is linked to heart disease, and heart attacks. Coronary arteries deliver oxygen-rich blood to the heart muscle. Reduced blood flow to the heart associated with coronary ischemia can result in inadequate oxygen supply to the heart muscle. When oxygen supply to the heart is unable to keep up with oxygen demand from the muscle, the result is the characteristic symptoms of coronary ischemia, the most common of which is chest pain. Chest pain due to coronary ischemia commonly radiates to the arm or neck. Certain individuals such as women, diabetics, and the elderly may present with more varied symptoms. If blood flow through the coronary arteries is stopped completely, cardiac muscle cells may die, known as a myocardial infarction, or heart attack.
Spontaneous coronary artery dissection (SCAD) is an uncommon but potentially lethal condition in which one of the coronary arteries that supply the heart, spontaneously develops a blood collection, or hematoma, within the artery wall due to a tear in the wall. SCAD is one of the arterial dissections that can occur.
A panoramic radiograph is a panoramic scanning dental X-ray of the upper and lower jaw. It shows a two-dimensional view of a half-circle from ear to ear. Panoramic radiography is a form of focal plane tomography; thus, images of multiple planes are taken to make up the composite panoramic image, where the maxilla and mandible are in the focal trough and the structures that are superficial and deep to the trough are blurred.
The BaleDoneen Method is a risk assessment and treatment protocol aimed at preventing heart attack and stroke. The method also seeks to prevent or reduce the effects of type 2 diabetes. The method was developed by Bradley Field Bale and Amy Doneen.
Blood vessel disorder generally refers to the narrowing, hardening or enlargement of arteries and veins. It is often due to the build-up of fatty deposits in the lumen of blood vessels or infection of the vessel wall. This can occur in various locations such as coronary blood vessels, peripheral arteries and veins. The narrowed arteries would block the blood supply to different organs and tissues. In severe conditions, it may develop into more critical health problems like myocardial infarction, stroke or heart failure, which are some of the major reasons of death.
Arterial occlusion is a condition involving partial or complete blockage of blood flow through an artery. Arteries are blood vessels that carry oxygenated blood to body tissues. An occlusion of arteries disrupts oxygen and blood supply to tissues, leading to ischemia. Depending on the extent of ischemia, symptoms of arterial occlusion range from simple soreness and pain that can be relieved with rest, to a lack of sensation or paralysis that could require amputation.
1 2 3 4 5 Glagov, Seymour; Weisenberg, Elliot; Zarins, Christopher K.; Stankunavicius, Regina; Kolettis, George J. (28 May 1987). "Compensatory Enlargement of Human Atherosclerotic Coronary Arteries". New England Journal of Medicine. 316 (22): 1371–1375. doi:10.1056/NEJM198705283162204. PMID3574413.
Ornish, Dean (November 1998). "Avoiding revascularization with lifestyle changes: the multicenter lifestyle demonstration project". The American Journal of Cardiology. 82 (10): 72–76. doi:10.1016/s0002-9149(98)00744-9. PMID9860380.
Dod, Harvinder S.; Bhardwaj, Ravindra; Sajja, Venu; Weidner, Gerdi; Hobbs, Gerald R.; Konat, Gregory W.; Manivannan, Shanthi; Gharib, Wissam; Warden, Bradford E.; Nanda, Navin C.; Beto, Robert J.; Ornish, Dean; Jain, Abnash C. (February 2010). "Effect of Intensive Lifestyle Changes on Endothelial Function and on Inflammatory Markers of Atherosclerosis". The American Journal of Cardiology. 105 (3): 362–367. doi:10.1016/j.amjcard.2009.09.038. PMID20102949.
Silberman, Anna; Banthia, Rajni; Estay, Ivette S.; Kemp, Colleen; Studley, Joli; Hareras, Dennis; Ornish, Dean (March 2010). "The Effectiveness and Efficacy of an Intensive Cardiac Rehabilitation Program in 24 Sites". American Journal of Health Promotion. 24 (4): 260–266. doi:10.4278/ajhp.24.4.arb. PMID20232608. S2CID25915559.
Glagov, Seymour; Weisenberg, Elliot; Zarins, Christopher K.; Stankunavicius, Regina; Kolettis, George J. (28 May 1987). "Compensatory Enlargement of Human Atherosclerotic Coronary Arteries". New England Journal of Medicine. 316 (22): 1371–1375. doi:10.1056/NEJM198705283162204. PMID3574413.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.