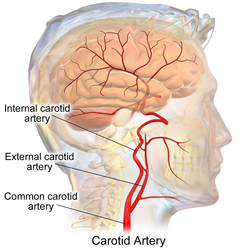
In human anatomy, the internal and external carotid arise from the common carotid artery, where it bifurcates at cervical vertebrae C3 or C4. The internal carotid artery supplies the brain, including the eyes,[2] while the external carotid nourishes other portions of the head, such as the face, scalp, skull, and meninges.
Classification
Terminologia Anatomica in 1998 subdivided the artery into four parts: "cervical", "petrous", "cavernous", and "cerebral".[3][4]
In clinical settings, however, usually the classification system of the internal carotid artery follows the 1996 recommendations by Bouthillier,[5] describing seven anatomical segments of the internal carotid artery, each with a corresponding alphanumeric identifier: C1 cervical; C2 petrous; C3 lacerum; C4 cavernous; C5 clinoid; C6 ophthalmic; and C7 communicating. The Bouthillier nomenclature remains in widespread use by neurosurgeons, neuroradiologists and neurologists.
The segments are subdivided based on anatomical and microsurgical landmarks and surrounding anatomy, more than angiographic appearance of the artery. An alternative embryologic classification system proposed by Pierre Lasjaunias[6] and colleagues is invaluable when it comes to explanation of many internal carotid artery variants. An older clinical classification, based on pioneering work by Fischer,[7] is mainly of historical significance.
Internal carotid artery
The segments of the internal carotid artery are as follows:
Cervical segment, or C1, identical to the commonly used cervical portion
Segments of the internal carotid artery, delineated on an MRA of the head.
The internal carotid artery is a terminal branch of the common carotid artery; it arises around the level of the fourth cervical vertebra when the common carotid bifurcates into this artery and its more superficial counterpart, the external carotid artery.
C1: Cervical segment
Level of 6th cervical vertebrae - still at level of common carotid but relationships are similar to those of cervical segment of internal carotid
The cervical segment, or C1, or cervical part of the internal carotid, extends from the carotid bifurcation until it enters the carotid canal in the skull anterior to the jugular foramen.
Internal carotid artery - dissection
At its origin, the internal carotid artery is somewhat dilated. This part of the artery is known as the carotid sinus or the carotid bulb. The ascending portion of the cervical segment occurs distal to the bulb when the vessel walls are again parallel.
The internal carotid runs vertically upward in the carotid sheath and enters the skull through the carotid canal. During this part of its course, it lies in front of the transverse processes of the upper three cervical vertebrae.
The petrous segment, or C2, of the internal carotid, is that which is inside the petrous part of the temporal bone. This segment extends until the foramen lacerum.
The petrous portion classically has three sections:
an ascending, or vertical, portion;
the genu, or bend; and
the horizontal portion.
When the internal carotid artery enters the canal in the petrous portion of the temporal bone, it first ascends a short distance and then curves anteriorly and medially. The artery lies at first in front of the cochlea and tympanic cavity; from the latter cavity it is separated by a thin, bony lamella, which is cribriform in the young subject, and often partly absorbed in old age. Farther forward, it is separated from the trigeminal ganglion by a thin plate of bone, which forms the floor of the fossa for the ganglion and the roof of the horizontal portion of the canal. Frequently this bony plate is more or less deficient, and then the ganglion is separated from the artery by fibrous membrane. The artery is separated from the bony wall of the carotid canal by a prolongation of dura mater and is surrounded by a number of small veins and by filaments of the carotid plexus, derived from the ascending branch of the superior cervical ganglion of the sympathetic trunk.
The named branches of the petrous segment of the internal carotid artery are:
The lacerum segment, or C3, is a short segment that begins above the foramen lacerum and ends at the petrolingual ligament, a reflection of periosteum between the lingula and petrous apex (or petrosal process) of the sphenoid bone. The lacerum portion is still considered "extradural" since it is surrounded by periosteum and fibrocartilage along its course. It is erroneously stated in several anatomy textbooks that the internal carotid artery passes through the foramen lacerum. This at best has only ever been a partial truth in that it passes through the superior part of the foramen on its way to the cavernous sinus. As such it does not traverse the skull through it. The inferior part of the foramen is actually filled with fibrocartilage. The broad consensus is that the internal carotid artery should not be described as travelling through the foramen lacerum.[8]
C4: Cavernous segment
Oblique section through the cavernous sinus.
The cavernous segment, or C4, of the internal carotid artery begins at the petrolingual ligament and extends to the proximal dural ring, which is formed by the medial and inferior periosteum of the anterior clinoid process. The cavernous segment is surrounded by the cavernous sinus.
In this part of its course, the artery is situated between the layers of the dura mater forming the cavernous sinus, but covered by the lining membrane of the sinus. It at first ascends toward the posterior clinoid process, then passes forward by the side of the body of the sphenoid bone, again curves upward on the medial side of the anterior clinoid process, and perforates the dura mater forming the roof of the sinus. The curve in the cavernous segment is called the carotid siphon. This portion of the artery is surrounded by filaments of the sympathetic trunk, and on its lateral side is the abducent nerve, or cranial nerve VI.
The cavernous segment also gives rise to small capsular arteries that supply the wall of the cavernous sinus.
C5: Clinoid segment
The clinoid segment, or C5, is another short segment of the internal carotid that begins after the artery exits the cavernous sinus at the proximal dural ring and extends distally to the distal dural ring, after which the carotid artery is considered "intra-dural" and has entered the subarachnoid space.
The clinoid segment normally has no named branches, though the ophthalmic artery may arise from the clinoid segment.
C6: Ophthalmic segment
The ophthalmic artery and its branches
The ophthalmic segment, or C6, extends from the distal dural ring, which is continuous with the falx cerebri, to the origin of the posterior communicating artery. The ophthalmic segment courses roughly horizontally, parallel to the optic nerve, which runs superomedially to the carotid at this point.
The communicating segment, or terminal segment, or C7, of the internal carotid artery passes between the optic and oculomotor nerves to the anterior perforated substance at the medial extremity of the lateral cerebral fissure. Angiographically, this segment extends from the origin of the posterior communicating artery to the bifurcation of the internal carotid artery.
The named branches of the communicating segment are:
Typically internal carotid artery blood flow velocities are measured in peak systolic velocity (PSV) and end diastolic velocity (EDV) and according to Society of Radiologists in Ultrasound in healthy subjects without stenosis must be below 125 cm/sec at PSV and below 40 cm/sec at EDV.[10]
One study found that for normative males in the 20-39 age group, PSV averaged 82 cm/sec and EDV 34 cm/sec. In the male 80+ age group, PSV averaged 76 cm/sec and EDV 18 cm/sec.[11]
Additional images
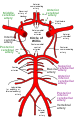
Circle of Willis
Diagram of the arterial circulation at the base of the brain (inferior view).
↑ Kiel JW (2010). "The Ocular Circulation". Integrated Systems Physiology: From Molecule to Function to Disease. 3: 1–81. doi:10.4199/C00024ED1V01Y201012ISP012. PMID21452447. The arterial input to the eye is provided by several branches from the ophthalmic artery, which is derived from the internal carotid artery in most mammals.
↑ Bouthillier, Alain; Harry van Loveren; Jefferey Keller (March 1996). "Segments of the internal carotid artery: a new classification". Neurosurgery. 38 (3): 425–432. doi:10.1097/00006123-199603000-00001. PMID8837792.
↑ Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: angiographic aspects with embryological discussion. Anat Clin 1984;6:133–41
↑ Fischer E. Die Lageabweichungen der vorderen Hirnarterie im Gefa¨ssbild. Zentralbl Neurochir 1938;3:300 –13
↑ TAUBER M, VAN LOVEREN H. R et al. The enigmatic foramen lacerum. Commentaries. Neurosurgery. 1999, vol. 44, no2, pp. 386-393
↑ Osborn, Anne (1999). Diagnostic Cerebral Angiography (2nded.). Philadelphia, PA, USA: Lippincott Williams & Wilkins. ISBN0-397-58404-0.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.