
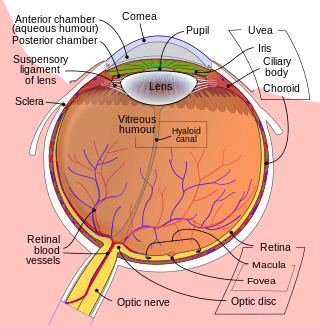
The cornea is the transparent front part of the eye that covers the iris, pupil, and anterior chamber. Along with the anterior chamber and lens, the cornea refracts light, accounting for approximately two-thirds of the eye's total optical power. In humans, the refractive power of the cornea is approximately 43 dioptres. The cornea can be reshaped by surgical procedures such as LASIK.

LASIK or Lasik, commonly referred to as laser eye surgery or laser vision correction, is a type of refractive surgery for the correction of myopia, hyperopia, and an actual cure for astigmatism, since it is in the cornea. LASIK surgery is performed by an ophthalmologist who uses a laser or microkeratome to reshape the eye's cornea in order to improve visual acuity. For most people, LASIK provides a long-lasting alternative to eyeglasses or contact lenses.

Photorefractive keratectomy (PRK) and laser-assisted sub-epithelial keratectomy (LASEK) are laser eye surgery procedures intended to correct a person's vision, reducing dependency on glasses or contact lenses. LASEK and PRK permanently change the shape of the anterior central cornea using an excimer laser to ablate a small amount of tissue from the corneal stroma at the front of the eye, just under the corneal epithelium. The outer layer of the cornea is removed prior to the ablation.

Radial keratotomy (RK) is a refractive surgical procedure to correct myopia (nearsightedness). It was developed in 1974 by Svyatoslav Fyodorov, a Russian ophthalmologist. It has been largely supplanted by newer operations, such as photorefractive keratectomy, LASIK, Epi-LASIK and the phakic intraocular lens. Approximately 10% of all practicing ophthalmologists in the United States have performed several hundred thousand RK procedures.
Refractive eye surgery is optional eye surgery used to improve the refractive state of the eye and decrease or eliminate dependency on glasses or contact lenses. This can include various methods of surgical remodeling of the cornea (keratomileusis), lens implantation or lens replacement. The most common methods today use excimer lasers to reshape the curvature of the cornea. Refractive eye surgeries are used to treat common vision disorders such as myopia, hyperopia, presbyopia and astigmatism.

The corneal endothelium is a single layer of endothelial cells on the inner surface of the cornea. It faces the chamber formed between the cornea and the iris.
Epi-LASIK is a refractive surgery technique designed to reduce a person's dependency on eyeglasses and contact lenses. Invented by Dr. Ioannis Pallikaris, the technique is basically an automatic LASEK without alcohol; it can be better considered as superficial LASIK. The stromal bed is smoother than that obtained by mechanical methods or brush. Unlike alcohol (LASEK), there is no chance of damaging the limbal stem cells. It is also relatively less painful than LASEK.
- A device similar to a microkeratome slides over the surface of the cornea, just underneath the epithelial layer of cells while suction is applied.
- The result is a hinged sheet of epithelium that is at least partially viable.
- It is reflected out of the way so that the ablation can take place.
- The sheet is repositioned and a bandage soft contact lens is placed on the eye.

Fuchs dystrophy, also referred to as Fuchs endothelial corneal dystrophy (FECD) and Fuchs endothelial dystrophy (FED), is a slowly progressing corneal dystrophy that usually affects both eyes and is slightly more common in women than in men. Although early signs of Fuchs dystrophy are sometimes seen in people in their 30s and 40s, the disease rarely affects vision until people reach their 50s and 60s.
Recurrent corneal erosion is a disorder of the eyes characterized by the failure of the cornea's outermost layer of epithelial cells to attach to the underlying basement membrane. The condition is excruciatingly painful because the loss of these cells results in the exposure of sensitive corneal nerves. This condition can often leave patients with temporary blindness due to extreme light sensitivity (photophobia).
Descemet's membrane is the basement membrane that lies between the corneal proper substance, also called stroma, and the endothelial layer of the cornea. It is composed of different kinds of collagen than the stroma. The endothelial layer is located at the posterior of the cornea. Descemet's membrane, as the basement membrane for the endothelial layer, is secreted by the single layer of squamous epithelial cells that compose the endothelial layer of the cornea.

A corneal ulcer, or ulcerative keratitis, is an inflammatory condition of the cornea involving loss of its outer layer. It is very common in dogs and is sometimes seen in cats. In veterinary medicine, the term corneal ulcer is a generic name for any condition involving the loss of the outer layer of the cornea, and as such is used to describe conditions with both inflammatory and traumatic causes.

Corneal dystrophy is a group of rare hereditary disorders characterised by bilateral abnormal deposition of substances in the transparent front part of the eye called the cornea.
The stroma of the cornea is a fibrous, tough, unyielding, perfectly transparent and the thickest layer of the cornea of the eye. It is between Bowman's membrane anteriorly, and Descemet's membrane posteriorly.
The corneal epithelium is made up of epithelial tissue and covers the front of the cornea. It acts as a barrier to protect the cornea, resisting the free flow of fluids from the tears, and prevents bacteria from entering the epithelium and corneal stroma.

Pellucid marginal degeneration (PMD) is a degenerative corneal condition, often confused with keratoconus. It typically presents with painless vision loss affecting both eyes. Rarely, it may cause acute vision loss with severe pain due to perforation of the cornea. It is typically characterized by a clear, bilateral thinning (ectasia) in the inferior and peripheral region of the cornea, although some cases affect only one eye. The cause of the disease remains unclear.

Meesmann corneal dystrophy (MECD) is a rare hereditary autosomal dominant disease that is characterized as a type of corneal dystrophy and a keratin disease. MECD is characterized by the formation of microcysts in the outermost layer of the cornea, known as the anterior corneal epithelium. The anterior corneal epithelium also becomes fragile. This usually affects both eyes rather than a single eye and worsens over time. There are two phenotypes, Meesmann corneal dystrophy 1 (MECD1) and Meesmann corneal dystrophy 2 (MECD2), which affect the genes KRT3 and KRT12, respectively. A heterozygous mutation in either of these genes will lead to a single phenotype. Many with Meesmann corneal dystrophy are asymptomatic or experience mild symptoms.
The ocular immune system protects the eye from infection and regulates healing processes following injuries. The interior of the eye lacks lymph vessels but is highly vascularized, and many immune cells reside in the uvea, including mostly macrophages, dendritic cells, and mast cells. These cells fight off intraocular infections, and intraocular inflammation can manifest as uveitis or retinitis. The cornea of the eye is immunologically a very special tissue. Its constant exposure to the exterior world means that it is vulnerable to a wide range of microorganisms while its moist mucosal surface makes the cornea particularly susceptible to attack. At the same time, its lack of vasculature and relative immune separation from the rest of the body makes immune defense difficult. Lastly, the cornea is a multifunctional tissue. It provides a large part of the eye's refractive power, meaning it has to maintain remarkable transparency, but must also serve as a barrier to keep pathogens from reaching the rest of the eye, similar to function of the dermis and epidermis in keeping underlying tissues protected. Immune reactions within the cornea come from surrounding vascularized tissues as well as innate immune responsive cells that reside within the cornea.
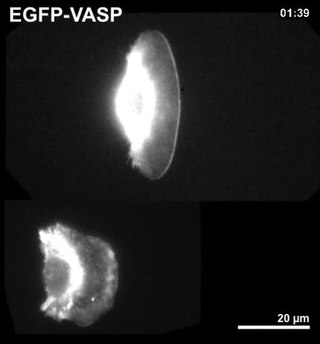
Corneal keratocytes are specialized fibroblasts residing in the stroma. This corneal layer, representing about 85-90% of corneal thickness, is built up from highly regular collagenous lamellae and extracellular matrix components. Keratocytes play the major role in keeping it transparent, healing its wounds, and synthesizing its components. In the unperturbed cornea keratocytes stay dormant, coming into action after any kind of injury or inflammation. Some keratocytes underlying the site of injury, even a light one, undergo apoptosis immediately after the injury. Any glitch in the precisely orchestrated process of healing may cloud the cornea, while excessive keratocyte apoptosis may be a part of the pathological process in the degenerative corneal disorders such as keratoconus, and these considerations prompt the ongoing research into the function of these cells.
Peter S. Hersh is an American ophthalmologist and specialist in LASIK eye surgery, keratoconus, and diseases of the cornea. He co-authored the article in the journal Ophthalmology that presented the results of the study that led to the first approval by the U.S. Food and Drug Administration (FDA) of the excimer laser for the correction of nearsightedness in the United States. Hersh was also medical monitor of the study that led to approval of corneal collagen crosslinking for the treatment of keratoconus.

The human cornea is a transparent membrane which allows light to pass through it. The word corneal opacification literally means loss of normal transparency of cornea. The term corneal opacity is used particularly for the loss of transparency of cornea due to scarring. Transparency of the cornea is dependent on the uniform diameter and the regular spacing and arrangement of the collagen fibrils within the stroma. Alterations in the spacing of collagen fibrils in a variety of conditions including corneal edema, scars, and macular corneal dystrophy is clinically manifested as corneal opacity. The term corneal blindness is commonly used to describe blindness due to corneal opacity.

{kind=link}