| Head and neck cancer | |
|---|---|
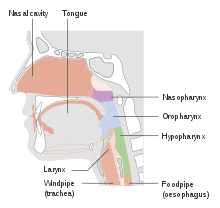 | |
| Parts of the head and neck that can be affected by cancer. | |
| Specialty | Oncology, oral and maxillofacial surgery |
| Symptoms | Lump or sore that does not heal, sore throat that does not go away, trouble swallowing, change in voice [1] |
| Risk factors | Alcohol, tobacco, betel quid, human papillomavirus, radiation exposure, certain workplace exposures, Epstein–Barr virus [1] [2] |
| Diagnostic method | Tissue biopsy [1] |
| Prevention | Not using tobacco or alcohol [2] |
| Treatment | Surgery, radiation therapy, chemotherapy, targeted therapy [1] |
| Frequency | 5.5 million (affected during 2015) [3] |
| Deaths | 379,000 (2015) [4] |
Head and neck cancer develops from tissues in the lip and oral cavity (mouth), larynx (throat), salivary glands, nose, sinuses, or skin of the face. [5] The most common types of head and neck cancer occur in the lips, mouth, and larynx. [5] Symptoms predominantly include a sore that does not heal or a change in the voice. [1] In those with advanced disease, there may be unusual bleeding, facial pain, numbness or swelling, and visible lumps on the outside of the neck or oral cavity. Given the location of these cancers, it is possible for an afflicted individual to experience difficulty breathing. [6]
Contents
- Signs and symptoms
- Mouth
- Nose
- Nasopharynx
- Throat
- Hypopharynx
- Larynx
- Trachea and salivary glands
- Causes
- Alcohol and tobacco
- Diet
- Betel nut
- Genetics
- Radiation
- Infection
- Gastroesophageal reflux disease
- Hematopoietic stem cell transplantation
- Other risk factors
- Diagnosis
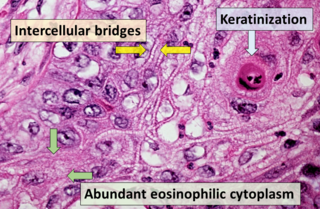
- Histopathology
- Prevention
- Management
- Surgery
- Radiation therapy
- Chemotherapy
- Photodynamic therapy
- Targeted therapy
- Immunotherapy
- Treatment side effects
- Psychosocial
- Prognosis
- Problem of second primaries
- Digestive system
- Mental health
- Others
- Epidemiology
- Research
- References
- External links
The majority of head and neck cancer is caused by the use of alcohol or tobacco, including smokeless tobacco, with increasing cases linked to the human papillomavirus (HPV). [6] [2] Other risk factors include the Epstein–Barr virus, betel quid, radiation exposure, and certain workplace exposures. [6] About 90% are pathologically classified as squamous cell cancers. [7] [2] The diagnosis is confirmed by a tissue biopsy. [6] The degree of surrounding tissue invasion and distant spread may be determined by medical imaging and blood tests. [6]
Not using tobacco or alcohol can reduce the risk of head and neck cancer. [2] The HPV vaccine may reduce the lifetime risk of oral cancer if taken prior to the onset of sexual activity, but confirmation will likely not be known until around 2060. [8] This is because oropharyngeal cancer typically presents in the 4th–6th decade of life, and this is a relatively new vaccine. While screening in the general population does not appear to be useful, screening high-risk groups by examination of the throat might be useful. [2] Head and neck cancer is often curable if it is diagnosed early; however, outcomes are typically poor if it is diagnosed late. [2] Treatment may include a combination of surgery, radiation therapy, chemotherapy, and targeted therapy. [6] Previous diagnosis and treatment of a head and neck cancer confer a higher risk of developing a second head and neck cancer or recurrence. [6]
Globally, head and neck cancer accounts for 650,000 new cases of cancer and 330,000 deaths annually on average. In 2018, it was the seventh most common cancer worldwide, with 890,000 new cases documented and 450,000 people dying from the disease. [8] In the United States, head and neck cancer makes up 3% of all cancer cases (averaging 53,000 new diagnoses per year) and 1.5% of cancer deaths. [9] The 2017 worldwide figure cites head and neck cancers as representing 5.3% of all cancers (not including non-melanoma skin cancers). [10] [5] Notably, head and neck cancer secondary to chronic alcohol or tobacco use has been steadily declining as less of the population chronically smokes tobacco. [8] However, HPV-associated oropharyngeal cancer is rising, particularly in younger people in westernized nations, which is thought to be reflective of changes in oral sexual practices, specifically with regard to the number of oral sexual partners. [5] [8] This increase since the 1970s has mostly affected wealthier nations and male populations. [11] [12] [5] This is due to evidence suggesting that transmission rates of HPV from women to men are higher than from men to women, as women often have a higher immune response to infection. [5] [13]
The usual age at diagnosis is between 55 and 65 years old. [14] The average 5-year survival following diagnosis in the developed world is 42–64%. [14] [15]