In neuroanatomy, the optic nerve, also known as the second cranial nerve, cranial nerve II, or simply CN II, is a paired cranial nerve that transmits visual information from the retina to the brain. In humans, the optic nerve is derived from optic stalks during the seventh week of development and is composed of retinal ganglion cell axons and glial cells; it extends from the optic disc to the optic chiasma and continues as the optic tract to the lateral geniculate nucleus, pretectal nuclei, and superior colliculus.
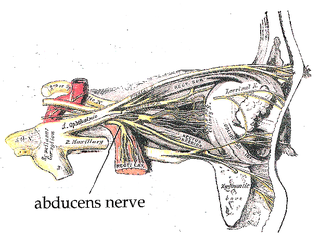
The abducens nerve or abducent nerve, also known as the sixth cranial nerve, cranial nerve VI, or simply CN VI, is a cranial nerve in humans and various other animals that controls the movement of the lateral rectus muscle, one of the extraocular muscles responsible for outward gaze. It is a somatic efferent nerve.
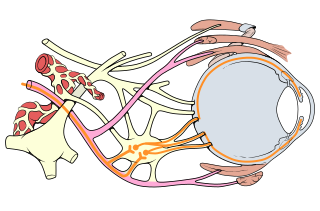
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
The trochlear nerve, also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye. Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve.

In anatomy, the orbit is the cavity or socket/hole of the skull in which the eye and its appendages are situated. "Orbit" can refer to the bony socket, or it can also be used to imply the contents. In the adult human, the volume of the orbit is 30 millilitres, of which the eye occupies 6.5 ml. The orbital contents comprise the eye, the orbital and retrobulbar fascia, extraocular muscles, cranial nerves II, III, IV, V, and VI, blood vessels, fat, the lacrimal gland with its sac and duct, the eyelids, medial and lateral palpebral ligaments, cheek ligaments, the suspensory ligament, septum, ciliary ganglion and short ciliary nerves.
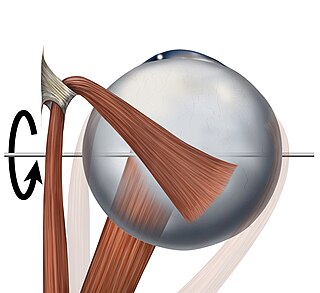
The superior oblique muscle or obliquus oculi superior is a fusiform muscle originating in the upper, medial side of the orbit which abducts, depresses and internally rotates the eye. It is the only extraocular muscle innervated by the trochlear nerve.

Duane syndrome is a congenital rare type of strabismus most commonly characterized by the inability of the eye to move outward. The syndrome was first described by ophthalmologists Jakob Stilling (1887) and Siegmund Türk (1896), and subsequently named after Alexander Duane, who discussed the disorder in more detail in 1905.

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.

The superior rectus muscle is a muscle in the orbit. It is one of the extraocular muscles. It is innervated by the superior division of the oculomotor nerve (III). In the primary position, its primary function is elevation, although it also contributes to intorsion and adduction. It is associated with a number of medical conditions, and may be weak, paralysed, overreactive, or even congenitally absent in some people.
The inferior rectus muscle is a muscle in the orbit near the eye. It is one of the four recti muscles in the group of extraocular muscles. It originates from the common tendinous ring, and inserts into the anteroinferior surface of the eye. It depresses the eye (downwards).
The medial rectus muscle is a muscle in the orbit near the eye. It is one of the extraocular muscles. It originates from the common tendinous ring, and inserts into the anteromedial surface of the eye. It is supplied by the inferior division of the oculomotor nerve (III). It rotates the eye medially (adduction).
The inferior oblique muscle or obliquus oculi inferior is a thin, narrow muscle placed near the anterior margin of the floor of the orbit. The inferior oblique is one of the extraocular muscles, and is attached to the maxillary bone (origin) and the posterior, inferior, lateral surface of the eye (insertion). The inferior oblique is innervated by the inferior branch of the oculomotor nerve.

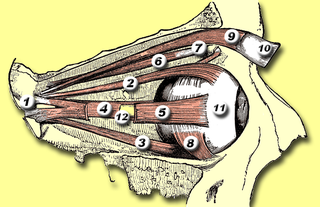
The extraocular muscles, or extrinsic ocular muscles, are the seven extrinsic muscles of the eye in humans and other animals. Six of the extraocular muscles, the four recti muscles, and the superior and inferior oblique muscles, control movement of the eye. The other muscle, the levator palpebrae superioris, controls eyelid elevation. The actions of the six muscles responsible for eye movement depend on the position of the eye at the time of muscle contraction.

The abducens nucleus is the originating nucleus from which the abducens nerve (VI) emerges—a cranial nerve nucleus. This nucleus is located beneath the fourth ventricle in the caudal portion of the pons near the midline, medial to the sulcus limitans.

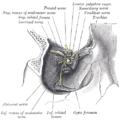
The superior orbital fissure is a foramen or cleft of the skull between the lesser and greater wings of the sphenoid bone. It gives passage to multiple structures, including the oculomotor nerve, trochlear nerve, ophthalmic nerve, abducens nerve, ophthalmic veins, and sympathetic fibres from the cavernous plexus.

Sixth nerve palsy, or abducens nerve palsy, is a disorder associated with dysfunction of cranial nerve VI, which is responsible for causing contraction of the lateral rectus muscle to abduct the eye. The inability of an eye to turn outward, results in a convergent strabismus or esotropia of which the primary symptom is diplopia in which the two images appear side-by-side. Thus, the diplopia is horizontal and worse in the distance. Diplopia is also increased on looking to the affected side and is partly caused by overaction of the medial rectus on the unaffected side as it tries to provide the extra innervation to the affected lateral rectus. These two muscles are synergists or "yoke muscles" as both attempt to move the eye over to the left or right. The condition is commonly unilateral but can also occur bilaterally.

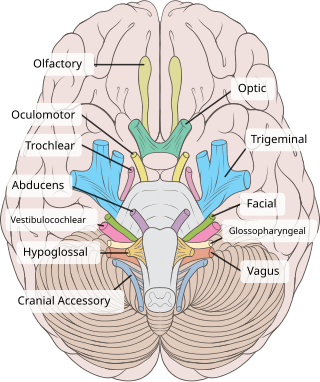
The cranial nerve exam is a type of neurological examination. It is used to identify problems with the cranial nerves by physical examination. It has nine components. Each test is designed to assess the status of one or more of the twelve cranial nerves (I-XII). These components correspond to testing the sense of smell (I), visual fields and acuity (II), eye movements and pupils, sensory function of face (V), strength of facial (VII) and shoulder girdle muscles (XI), hearing and balance, taste, pharyngeal movement and reflex, tongue movements (XII).
Oculomotor nerve palsy or oculomotor neuropathy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Damage to this nerve will result in an inability to move the eye normally. The nerve also supplies the upper eyelid muscle and is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movement resulting from the condition are generally so severe that patients are often unable to maintain normal eye alignment when gazing straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).
The term gaze is frequently used in physiology to describe coordinated motion of the eyes and neck. The lateral gaze is controlled by the paramedian pontine reticular formation (PPRF). The vertical gaze is controlled by the rostral interstitial nucleus of medial longitudinal fasciculus and the interstitial nucleus of Cajal.
Alternating hemiplegia is a form of hemiplegia that has an ipsilateral cranial nerve palsies and contralateral hemiplegia or hemiparesis of extremities of the body. The disorder is characterized by recurrent episodes of paralysis on one side of the body. There are multiple forms of alternating hemiplegia, Weber's syndrome, middle alternating hemiplegia, and inferior alternating hemiplegia. This type of syndrome can result from a unilateral lesion in the brainstem affecting both upper motor neurons and lower motor neurons. The muscles that would receive signals from these damaged upper motor neurons result in spastic paralysis. With a lesion in the brainstem, this affects the majority of limb and trunk muscles on the contralateral side due to the upper motor neurons decussation after the brainstem. The cranial nerves and cranial nerve nuclei are also located in the brainstem making them susceptible to damage from a brainstem lesion. Cranial nerves III (Oculomotor), VI (Abducens), and XII (Hypoglossal) are most often associated with this syndrome given their close proximity with the pyramidal tract, the location which upper motor neurons are in on their way to the spinal cord. Damages to these structures produce the ipsilateral presentation of paralysis or palsy due to the lack of cranial nerve decussation before innervating their target muscles. The paralysis may be brief or it may last for several days, many times the episodes will resolve after sleep. Some common symptoms of alternating hemiplegia are mental impairment, gait and balance difficulties, excessive sweating and changes in body temperature.