
Interstitial cystitis (IC), a type of bladder pain syndrome (BPS), is chronic pain in the bladder and pelvic floor of unknown cause. It is the urologic chronic pelvic pain syndrome of women. Symptoms include feeling the need to urinate right away, needing to urinate often, and pain with sex. IC/BPS is associated with depression and lower quality of life. Many of those affected also have irritable bowel syndrome and fibromyalgia.

Endometriosis is a disease of the female reproductive system in which cells similar to those in the endometrium, the layer of tissue that normally covers the inside of the uterus, grow outside the uterus. Lesions can be found on ovaries, fallopian tubes, tissue around the uterus and ovaries (peritoneum), intestines, bladder, and diaphragm; it may also occur in other parts of the body. Some symptoms include pelvic pain, heavy and painful periods, pain with bowel movements, painful urination, pain during sexual intercourse and infertility. Nearly half of those affected have chronic pelvic pain, while in 70% pain occurs during menstruation. Infertility occurs in up to half of affected individuals. About 25% of individuals have no symptoms and 85% of those seen with infertility in a tertiary center have no pain. Endometriosis can have both social and psychological effects.

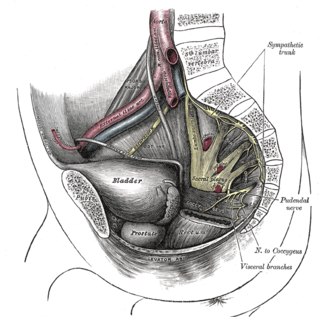
The pudendal nerve is the main nerve of the perineum. It is a mixed nerve and also conveys sympathetic autonomic fibers. It carries sensation from the external genitalia of both sexes and the skin around the anus and perineum, as well as the motor supply to various pelvic muscles, including the male or female external urethral sphincter and the external anal sphincter.

Sciatica is pain going down the leg from the lower back. This pain may go down the back, outside, or front of the leg. Onset is often sudden following activities like heavy lifting, though gradual onset may also occur. The pain is often described as shooting. Typically, symptoms are only on one side of the body. Certain causes, however, may result in pain on both sides. Lower back pain is sometimes present. Weakness or numbness may occur in various parts of the affected leg and foot.
Pudendal nerve entrapment (PNE), also known as Alcock canal syndrome, is an uncommon source of chronic pain in which the pudendal nerve is entrapped or compressed in Alcock's canal. There are several different types of PNE based on the site of entrapment anatomically. Pain is positional and is worsened by sitting. Other symptoms include genital numbness, fecal incontinence and urinary incontinence.

A spinal cord stimulator (SCS) or dorsal column stimulator (DCS) is a type of implantable neuromodulation device that is used to send electrical signals to select areas of the spinal cord for the treatment of certain pain conditions. SCS is a consideration for people who have a pain condition that has not responded to more conservative therapy. There are also spinal cord stimulators under research and development that could enable patients with spinal cord injury to walk again via epidural electrical stimulation (EES).
A neurectomy, or nerve resection is a neurosurgical procedure in which a peripheral nerve is cut or removed to alleviate neuropathic pain or permanently disable some function of a nerve. The nerve is not intended to grow back. For chronic pain it may be an alternative to a failed nerve decompression when the target nerve has no motor function and numbness is acceptable. Neurectomies have also been used to permanently block autonomic function, and special sensory function not related to pain.
Tethered cord syndrome (TCS) refers to a group of neurological disorders that relate to malformations of the spinal cord. Various forms include tight filum terminale, lipomeningomyelocele, split cord malformations (diastematomyelia), occult, dermal sinus tracts, and dermoids. All forms involve the pulling of the spinal cord at the base of the spinal canal, literally a tethered cord. The spinal cord normally hangs loose in the canal, free to move up and down with growth, and with bending and stretching. A tethered cord, however, is held taut at the end or at some point in the spinal canal. In children, a tethered cord can force the spinal cord to stretch as they grow. In adults the spinal cord stretches in the course of normal activity, usually leading to progressive spinal cord damage if untreated. TCS is often associated with the closure of a spina bifida. It can be congenital, such as in tight filum terminale, or the result of injury later in life.
Sacral nerve stimulation, also termed sacral neuromodulation, is a type of medical electrical stimulation therapy.
Responsive neurostimulation device is a medical device that senses changes in a person's body and uses neurostimulation to respond in the treatment of disease. The FDA has approved devices for use in the United States in the treatment of epileptic seizures and chronic pain conditions. Devices are being studied for use in the treatment of essential tremor, Parkinson's disease, Tourette's syndrome, depression, obesity, and post-traumatic stress disorder.

Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), previously known as chronic nonbacterial prostatitis, is long-term pelvic pain and lower urinary tract symptoms (LUTS) without evidence of a bacterial infection. It affects about 2–6% of men. Together with IC/BPS, it makes up urologic chronic pelvic pain syndrome (UCPPS).

Nerve compression syndrome, or compression neuropathy, or nerve entrapment syndrome, is a medical condition caused by chronic, direct pressure on a peripheral nerve. It is known colloquially as a trapped nerve, though this may also refer to nerve root compression. Its symptoms include pain, tingling, numbness and muscle weakness. The symptoms affect just one particular part of the body, depending on which nerve is affected. The diagnosis is largely clinical and can be confirmed with diagnostic nerve blocks. Occasionally imaging and electrophysiology studies aid in the diagnosis. Timely diagnosis is important as untreated chronic nerve compression may cause permanent damage. A surgical nerve decompression can relieve pressure on the nerve but cannot always reverse the physiological changes that occurred before treatment. Nerve injury by a single episode of physical trauma is in one sense an acute compression neuropathy but is not usually included under this heading, as chronic compression takes a unique pathophysiological course.
Visceral pain is pain that results from the activation of nociceptors of the thoracic, pelvic, or abdominal viscera (organs). Visceral structures are highly sensitive to distension (stretch), ischemia and inflammation, but relatively insensitive to other stimuli that normally evoke pain such as cutting or burning. Visceral pain is diffuse, difficult to localize and often referred to a distant, usually superficial, structure. It may be accompanied by symptoms such as nausea, vomiting, changes in vital signs as well as emotional manifestations. The pain may be described as sickening, deep, squeezing, and dull. Distinct structural lesions or biochemical abnormalities explain this type of pain in only a proportion of patients. These diseases are grouped under gastrointestinal neuromuscular diseases (GINMD). Others can experience occasional visceral pains, often very intense in nature, without any evidence of structural, biochemical or histolopathologic reason for such symptoms. These diseases are grouped under functional gastrointestinal disorders (FGID) and the pathophysiology and treatment can vary greatly from GINMD. The two major single entities among functional disorders of the gut are functional dyspepsia and irritable bowel syndrome.
Neuromodulation is "the alteration of nerve activity through targeted delivery of a stimulus, such as electrical stimulation or chemical agents, to specific neurological sites in the body". It is carried out to normalize – or modulate – nervous tissue function. Neuromodulation is an evolving therapy that can involve a range of electromagnetic stimuli such as a magnetic field (rTMS), an electric current, or a drug instilled directly in the subdural space. Emerging applications involve targeted introduction of genes or gene regulators and light (optogenetics), and by 2014, these had been at minimum demonstrated in mammalian models, or first-in-human data had been acquired. The most clinical experience has been with electrical stimulation.

Konstantin Slavin is a Professor and Head of the Department of Stereotactic and functional neurosurgery at the University of Illinois College of Medicine. He is a former president of the American Society for Stereotactic and functional neurosurgery and current vice-president of the World Society for Stereotactic and Functional Neurosurgery. His specialties include Aneurysm, Brain surgery, Brain Tumor, Cerebrovascular Disorders, Craniotomy, Dystonia, Essential Tremor, Facial Nerve Pain, Facial Pain, Glioblastoma, Headache disorders, Laminectomy, Lower back pain, Movement Disorders, Multiple Sclerosis, Neck Pain, Neurosurgery, Neurosurgical Procedures, Pain, Parkinson Disease, Spinal Cord Injuries, and Stroke.
Fowler's syndrome is a rare disorder in which the urethral sphincter fails to relax to allow urine to be passed normally in younger women with abnormal electromyographic activity detected.
Hard flaccid syndrome (HFS), also known as hard flaccid (HF), is a chronic painful condition characterized by a semi-rigid penis at the flaccid state, a soft glans at the erect state (cold glans syndrome), pelvic pain, low libido, erectile dysfunction, erectile pain, pain on ejaculation, penile sensory changes (numbness or coldness), lower urinary tract symptoms, contraction of the pelvic floor muscles, and psychological distress. Other complaints include rectal and perineal discomfort, cold hands and feet, and a hollow or detached feeling inside the penile shaft. The majority of HFS patients are in their 20s–30s and symptoms significantly affect one's quality of life.
Urologic chronic pelvic pain syndrome (UCPPS) is ongoing bladder pain in either sex, chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) in men and interstitial cystitis or painful bladder syndrome (IC/PBS) in women.
Pelvic floor physical therapy (PFPT) is a specialty area within physical therapy focusing on the rehabilitation of muscles in the pelvic floor after injury or dysfunction. It can be used to address issues such as muscle weakness or tightness post childbirth, dyspareunia, vaginismus, vulvodynia, constipation, fecal or urinary incontinence, pelvic organ prolapse, and sexual dysfunction. Licensed physical therapists with specialized pelvic floor physical therapy training address dysfunction in individuals across the gender and sex spectra, though PFPT often associated with women's health for its heavy focus on addressing issues of pelvic trauma after childbirth.
