
A lipoprotein is a biochemical assembly whose primary function is to transport hydrophobic lipid molecules in water, as in blood plasma or other extracellular fluids. They consist of a triglyceride and cholesterol center, surrounded by a phospholipid outer shell, with the hydrophilic portions oriented outward toward the surrounding water and lipophilic portions oriented inward toward the lipid center. A special kind of protein, called apolipoprotein, is embedded in the outer shell, both stabilising the complex and giving it a functional identity that determines its role.

Lysosomal storage diseases are a group of over 70 rare inherited metabolic disorders that result from defects in lysosomal function. Lysosomes are sacs of enzymes within cells that digest large molecules and pass the fragments on to other parts of the cell for recycling. This process requires several critical enzymes. If one of these enzymes is defective due to a mutation, the large molecules accumulate within the cell, eventually killing it.

Niemann–Pick disease is a group of severe inherited metabolic disorders, in which sphingomyelin accumulates in lysosomes in cells.

Glycogen storage disease type II, also called Pompe disease, and formerly known as GSD-IIa. It is an autosomal recessive metabolic disorder which damages muscle and nerve cells throughout the body. It is caused by an accumulation of glycogen in the lysosome due to deficiency of the lysosomal acid alpha-glucosidase enzyme. GSD-II and Danon disease are the only glycogen storage diseases with a defect in lysosomal metabolism, and Pompe disease was the first glycogen storage disease to be identified, in 1932 by the Dutch pathologist J. C. Pompe.
Inborn errors of metabolism form a large class of genetic diseases involving congenital disorders of enzyme activities. The majority are due to defects of single genes that code for enzymes that facilitate conversion of various substances (substrates) into others (products). In most of the disorders, problems arise due to accumulation of substances which are toxic or interfere with normal function, or due to the effects of reduced ability to synthesize essential compounds. Inborn errors of metabolism are now often referred to as congenital metabolic diseases or inherited metabolic disorders. To this concept it's possible to include the new term of Enzymopathy. This term was created following the study of Biodynamic Enzymology, a science based on the study of the enzymes and their derivated products. Finally, inborn errors of metabolism were studied for the first time by British physician Archibald Garrod (1857–1936), in 1908. He is known for work that prefigured the "one gene-one enzyme" hypothesis, based on his studies on the nature and inheritance of alkaptonuria. His seminal text, Inborn Errors of Metabolism, was published in 1923.
Hyperlipidemia is abnormally elevated levels of any or all lipids or lipoproteins in the blood. The term hyperlipidemia refers to the laboratory finding itself and is also used as an umbrella term covering any of various acquired or genetic disorders that result in that finding. Hyperlipidemia represents a subset of dyslipidemia and a superset of hypercholesterolemia. Hyperlipidemia is usually chronic and requires ongoing medication to control blood lipid levels.
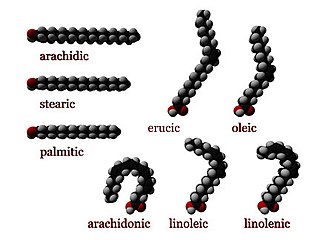
Numerous genetic disorders are caused by errors in fatty acid metabolism. These disorders may be described as fatty oxidation disorders or as a lipid storage disorders, and are any one of several inborn errors of metabolism that result from enzyme defects affecting the ability of the body to oxidize fatty acids in order to produce energy within muscles, liver, and other cell types.
Progressive familial intrahepatic cholestasis (PFIC) is a group of familial cholestatic conditions caused by defects in biliary epithelial transporters. The clinical presentation usually occurs first in childhood with progressive cholestasis. This usually leads to failure to thrive, cirrhosis, and the need for liver transplantation.

Lecithin–cholesterol acyltransferase is an enzyme, in many animals including humans, that converts free cholesterol into cholesteryl ester, which is then sequestered into the core of a lipoprotein particle, eventually making the newly synthesized HDL spherical and forcing the reaction to become unidirectional since the particles are removed from the surface. The enzyme is bound to high-density lipoproteins (HDLs) (alpha-LCAT) and LDLs (beta-LCAT) in the blood plasma. LCAT deficiency can cause impaired vision due to cholesterol corneal opacities, anemia, and kidney damage. It belongs to the family of phospholipid:diacylglycerol acyltransferases.

Familial hypercholesterolemia (FH) is a genetic disorder characterized by high cholesterol levels, specifically very high levels of low-density lipoprotein cholesterol, in the blood and early cardiovascular diseases. The most common mutations diminish the number of functional LDL receptors in the liver or produce abnormal LDL receptors that never go to the cell surface to function properly. Since the underlying body biochemistry is slightly different in individuals with FH, their high cholesterol levels are less responsive to the kinds of cholesterol control methods which are usually more effective in people without FH. Nevertheless, treatment is usually effective.
Acid lipase disease or deficiency is a name used to describe two related disorders of fatty acid metabolism. Acid lipase disease occurs when the enzyme lysosomal acid lipase that is needed to break down certain fats that are normally digested by the body is lacking or missing. This results in the toxic buildup of these fats in the body's cells and tissues. These fatty substances, called lipids, include waxes, oils, and cholesterol.
Lecithin cholesterol acyltransferase deficiency is a disorder of lipoprotein metabolism. The disease has two forms: Familial LCAT deficiency, in which there is complete LCAT deficiency, and Fish-eye disease, in which there is a partial deficiency.

Hormone-sensitive lipase (EC 3.1.1.79, HSL), also previously known as cholesteryl ester hydrolase (CEH), sometimes referred to as triacylglycerol lipase, is an enzyme that, in humans, is encoded by the LIPE gene, and catalyzes the following reaction:
Lysosomal lipase is a form of lipase which functions intracellularly, in the lysosomes.

Lipoprotein lipase deficiency is a genetic disorder in which a person has a defective gene for lipoprotein lipase, which leads to very high triglycerides, which in turn causes stomach pain and deposits of fat under the skin, and which can lead to problems with the pancreas and liver, which in turn can lead to diabetes. The disorder only occurs if a child acquires the defective gene from both parents. It is managed by restricting fat in diet to less than 20 g/day.
Hepatic lipase (HL), also called hepatic triglyceride lipase (HTGL) or LIPC (for "lipase, hepatic"), is a form of lipase, catalyzing the hydrolysis of triacylglyceride. Hepatic lipase is coded by chromosome 15 and its gene is also often referred to as HTGL or LIPC. Hepatic lipase is expressed mainly in liver cells, known as hepatocytes, and endothelial cells of the liver. The hepatic lipase can either remain attached to the liver or can unbind from the liver endothelial cells and is free to enter the body's circulation system. When bound on the endothelial cells of the liver, it is often found bound to heparan sulfate proteoglycans (HSPG), keeping HL inactive and unable to bind to HDL (high-density lipoprotein) or IDL (intermediate-density lipoprotein). When it is free in the bloodstream, however, it is found associated with HDL to maintain it inactive. This is because the triacylglycerides in HDL serve as a substrate, but the lipoprotein contains proteins around the triacylglycerides that can prevent the triacylglycerides from being broken down by HL.
Sterol O-acyltransferase is an intracellular protein located in the endoplasmic reticulum that forms cholesteryl esters from cholesterol.
Synageva BioPharma Corp. was a publicly listed biopharmaceutical company headquartered in Lexington, Massachusetts dedicated to discovering, developing and delivering medicines for patients with rare diseases and high unmet medical needs. The company had manufacturing and laboratory locations in Lexington and Holden, Massachusetts, Bogart and Athens Georgia, as well as offices in a variety of locations around the world.
Sebelipase alfa, sold under the brand name Kanuma, is a recombinant form of the enzyme lysosomal acid lipase (LAL) that is used as a medication for the treatment of lysosomal acid lipase deficiency (LAL-D). It is administered via intraveneous infusion. It was approved for medical use in the European Union and in the United States in 2015.

Lipase A, lysosomal acid type is a protein that in humans is encoded by the LIPA gene.
