Myasthenia gravis (MG) is a long-term neuromuscular junction disease that leads to varying degrees of skeletal muscle weakness. The most commonly affected muscles are those of the eyes, face, and swallowing. It can result in double vision, drooping eyelids, and difficulties in talking and walking. Onset can be sudden. Those affected often have a large thymus or develop a thymoma.
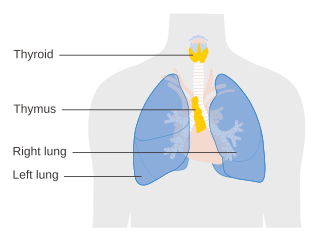
The thymus is a specialized primary lymphoid organ of the immune system. Within the thymus, thymus cell lymphocytes or T cells mature. T cells are critical to the adaptive immune system, where the body adapts to specific foreign invaders. The thymus is located in the upper front part of the chest, in the anterior superior mediastinum, behind the sternum, and in front of the heart. It is made up of two lobes, each consisting of a central medulla and an outer cortex, surrounded by a capsule.

Mesothelioma is a type of cancer that develops from the thin layer of tissue that covers many of the internal organs. The area most commonly affected is the lining of the lungs and chest wall. Less commonly the lining of the abdomen and rarely the sac surrounding the heart, or the sac surrounding the testis may be affected. Signs and symptoms of mesothelioma may include shortness of breath due to fluid around the lung, a swollen abdomen, chest wall pain, cough, feeling tired, and weight loss. These symptoms typically come on slowly.
A thymectomy is an operation to remove the thymus. It usually results in remission of myasthenia gravis with the help of medication including steroids. However, this remission may not be permanent. Thymectomy is indicated when thymoma are present in the thymus. Anecdotal evidence suggests MG patients with no evidence of thymoma may still benefit from thymectomy.

Surface epithelial-stromal tumors are a class of ovarian neoplasms that may be benign or malignant. Neoplasms in this group are thought to be derived from the ovarian surface epithelium or from ectopic endometrial or fallopian tube (tubal) tissue. Tumors of this type are also called ovarian adenocarcinoma. This group of tumors accounts for 90% to 95% of all cases of ovarian cancer; however is mainly only found in postmenopausal women with the exception of the United States where 7% of cases occur in women under the age of 40. Serum CA-125 is often elevated but is only 50% accurate so it is not a useful tumor marker to assess the progress of treatment. 75% of women with epithelial ovarian cancer are found within the advanced-stages; however younger patients are more likely to have better prognoses than older patients.

Pseudomyxoma peritonei (PMP) is a clinical condition caused by cancerous cells that produce abundant mucin or gelatinous ascites. The tumors cause fibrosis of tissues and impede digestion or organ function, and if left untreated, the tumors and mucin they produce will fill the abdominal cavity. This will result in compression of organs and will destroy the function of the colon, small intestine, stomach, or other organs. Prognosis with treatment in many cases is optimistic, but the disease is lethal if untreated, with death occurring via cachexia, bowel obstruction, or other types of complications.

Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).

Oligoastrocytomas are a subset of brain tumors that present with an appearance of mixed glial cell origin, astrocytoma and oligodendroglioma. However, the term "Oligoastrocytoma" is now considered obsolete by the National Comprehensive Cancer Network stating "the term should no longer be used as such morphologically ambiguous tumors can be reliably resolved into astrocytomas and oligodendrogliomas with molecular testing."

A hemangiopericytoma is a type of soft-tissue sarcoma that originates in the pericytes in the walls of capillaries. When inside the nervous system, although not strictly a meningioma tumor, it is a meningeal tumor with a special aggressive behavior. It was first characterized in 1942.

A mediastinal tumor is a tumor in the mediastinum, the cavity that separates the lungs from the rest of the chest. It contains the heart, esophagus, trachea, thymus, and aorta. The most common mediastinal masses are neurogenic tumors, usually found in the posterior mediastinum, followed by thymoma (15–20%) located in the anterior mediastinum. Lung cancer typically spreads to the lymph nodes in the mediastinum.

Mucoepidermoid carcinoma (MEC) is the most common type of minor salivary gland malignancy in adults. Mucoepidermoid carcinoma can also be found in other organs, such as bronchi, lacrimal sac, and thyroid gland.

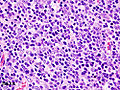
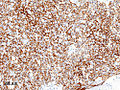
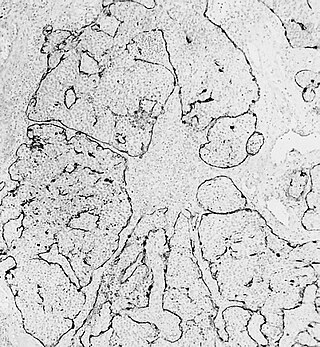
Thymic carcinoma, or type C thymoma, is a malignancy of the thymus. It is a rare cancer that is often diagnosed at advanced stages. Recurrence following treatment is common, and thymic carcinoma is associated with a poor prognosis.
Lung cancer staging is the assessment of the extent to which a lung cancer has spread from its original source. As with most cancers, staging is an important determinant of treatment and prognosis. In general, more advanced stages of cancer are less amenable to treatment and have a worse prognosis.
Esthesioneuroblastoma is a rare cancer of the nasal cavity. Arising from the upper nasal tract, esthesioneuroblastoma is believed to originate from sensory neuroepithelial cells, also known as neuroectodermal olfactory cells.
Thymus hyperplasia refers to an enlargement ("hyperplasia") of the thymus.

Philip Eugene Bernatz was an eminent American physician and thoracic surgeon at the Mayo Clinic, and an international authority on the diagnosis and treatment of thymoma and other tumors of the chest.

Intraperitoneal hyperthermic chemoperfusion is a type of hyperthermia therapy used in combination with surgery in the treatment of advanced abdominal cancers. In this procedure, warmed anti-cancer medications are infused and circulated in the peritoneal cavity (abdomen) for a short period of time. The chemotherapeutic agents generally infused during IPHC are mitomycin-C and cisplatin.
Ectopic thymus is a condition where thymus tissue is found in an abnormal location. It usually does not cause symptoms, but may leads to a mass in the neck that may compress the trachea and the esophagus. It is thought to be the result of either a failure of descent or a failure of involution of normal thymus tissue. It may be diagnosed with radiology, such as an ultrasound or magnetic resonance imaging. If it causes illness, surgery can be used to remove it. Recurrence after surgery is very unlikely.
Hyperthermic intrathoracic chemotherapy (HITOC) is part of a surgical strategy employed in the treatment of various pleural malignancies. The pleura in this situation could be considered to include the surface linings of the chest wall, lungs, mediastinum, and diaphragm. HITOC is the chest counterpart of HIPEC. Traditionally used in the treatment of malignant mesothelioma, a primary malignancy of the pleura, this modality has recently been evaluated in the treatment of secondary pleural malignancies.
Cytoreductive surgery (CRS) is a surgical procedure that aims to reduce the amount of cancer cells in the abdominal cavity for patients with tumors that have spread intraabdominally. It is often used to treat ovarian cancer but can also be used for other abdominal malignancies.