Myasthenia gravis (MG) is a long-term neuromuscular junction disease that leads to varying degrees of skeletal muscle weakness. The most commonly affected muscles are those of the eyes, face, and swallowing. It can result in double vision, drooping eyelids, and difficulties in talking and walking. Onset can be sudden. Those affected often have a large thymus or develop a thymoma.

The ovary is a gonad in the female reproductive system that produces ova. When an ovum is released, this travels through the fallopian tube/oviduct into the uterus. There is an ovary found on the left and the right side of the body. The ovaries also secrete hormones that play a role in the menstrual cycle and fertility. The ovary progresses through many stages beginning in the prenatal period through menopause. It is also an endocrine gland because of the various hormones that it secretes.
Menopause, also known as the climacteric, is the time when menstrual periods permanently stop, marking the end of reproduction. It typically occurs between the ages of 45 and 55, although the exact timing can vary. Menopause is usually a natural change. It can occur earlier in those who smoke tobacco. Other causes include surgery that removes both ovaries or some types of chemotherapy. At the physiological level, menopause happens because of a decrease in the ovaries' production of the hormones estrogen and progesterone. While typically not needed, a diagnosis of menopause can be confirmed by measuring hormone levels in the blood or urine. Menopause is the opposite of menarche, the time when a girl's periods start.

Polycystic ovary syndrome, or polycystic ovarian syndrome (PCOS), is the most common endocrine disorder in women of reproductive age. The syndrome is named after cysts which form on the ovaries of some people with this condition, though this is not a universal symptom, and not the underlying cause of the disorder.
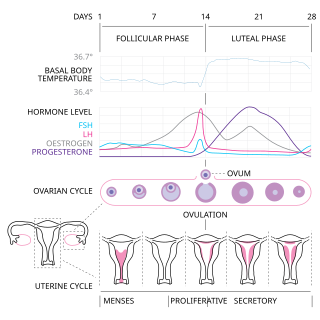
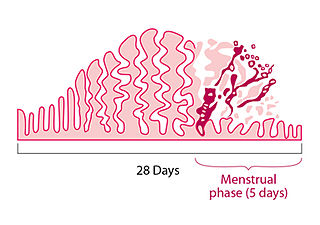
The menstrual cycle is a series of natural changes in hormone production and the structures of the uterus and ovaries of the female reproductive system that makes pregnancy possible. The ovarian cycle controls the production and release of eggs and the cyclic release of estrogen and progesterone. The uterine cycle governs the preparation and maintenance of the lining of the uterus (womb) to receive an embryo. These cycles are concurrent and coordinated, normally last between 21 and 35 days, with a median length of 28 days, and continue for about 30–45 years.
Amenorrhea is the absence of a menstrual period in a female who has reached reproductive age. Physiological states of amenorrhoea are seen, most commonly, during pregnancy and lactation (breastfeeding). Outside the reproductive years, there is absence of menses during childhood and after menopause.
Anovulation is when the ovaries do not release an oocyte during a menstrual cycle. Therefore, ovulation does not take place. However, a woman who does not ovulate at each menstrual cycle is not necessarily going through menopause. Chronic anovulation is a common cause of infertility.
Pubarche refers to the first appearance of pubic hair at puberty and it also marks the beginning of puberty. It is one of the physical changes of puberty and can occur independently of complete puberty. The early stage of sexual maturation, also known as adrenarche, is marked by characteristics including the development of pubic hair, axillary hair, adult apocrine body odor, acne, and increased oiliness of hair and skin. The Encyclopedia of Child and Adolescent Health corresponds SMR2 with pubarche, defining it as the development of pubic hair that occurs at a mean age of 11.6 years in females and 12.6 years in males. It further describes that pubarche's physical manifestation is vellus hair over the labia or the base of the penis. See Table 1 for the entirety of the sexual maturity rating description.
Ocular myasthenia gravis (MG) is a disease of the neuromuscular junction resulting in hallmark variability in muscle weakness and fatigability. MG is an autoimmune disease where anomalous antibodies are produced against the naturally occurring acetylcholine receptors in voluntary muscles. MG may be limited to the muscles of the eye, leading to abrupt onset of weakness/fatigability of the eyelids or eye movement. MG may also involve other muscle groups.
Hypoestrogenism, or estrogen deficiency, refers to a lower than normal level of estrogen. It is an umbrella term used to describe estrogen deficiency in various conditions. Estrogen deficiency is also associated with an increased risk of cardiovascular disease, and has been linked to diseases like urinary tract infections and osteoporosis.
A menstrual disorder is characterized as any abnormal condition with regards to a woman's menstrual cycle. There are many different types of menstrual disorders that vary with signs and symptoms, including pain during menstruation, heavy bleeding, or absence of menstruation. Normal variations can occur in menstrual patterns but generally menstrual disorders can also include periods that come sooner than 21 days apart, more than 3 months apart, or last more than 10 days in duration. Variations of the menstrual cycle are mainly caused by the immaturity of the hypothalamic-pituitary-ovarian (HPO) axis, and early detection and management is required in order to minimize the possibility of complications regarding future reproductive ability.
Primary ovarian insufficiency (POI), also called premature ovarian insufficiency, premature menopause, and premature ovarian failure, is the partial or total loss of reproductive and hormonal function of the ovaries before age 40 because of follicular dysfunction or early loss of eggs. POI can be seen as part of a continuum of changes leading to menopause that differ from age-appropriate menopause in the age of onset, degree of symptoms, and sporadic return to normal ovarian function. POI affects approximately 1 in 10,000 women under age 20, 1 in 1,000 women under age 30, and 1 in 100 of those under age 40. A medical triad for the diagnosis is amenorrhea, hypergonadotropism, and hypoestrogenism.
Paraneoplastic cerebellar degeneration (PCD) is a paraneoplastic syndrome associated with a broad variety of tumors including lung cancer, ovarian cancer, breast cancer, Hodgkin’s lymphoma and others. PCD is a rare condition that occurs in less than 1% of cancer patients.
Poor ovarian reserve is a condition of low fertility characterized by 1): low numbers of remaining oocytes in the ovaries or 2) possibly impaired preantral oocyte development or recruitment. Recent research suggests that premature ovarian aging and premature ovarian failure may represent a continuum of premature ovarian senescence. It is usually accompanied by high FSH levels.
Neuromuscular junction disease is a medical condition where the normal conduction through the neuromuscular junction fails to function correctly.
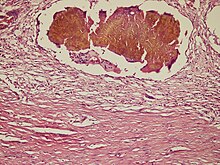
Theca lutein cyst is a type of bilateral functional ovarian cyst filled with clear, straw-colored fluid. These cysts result from exaggerated physiological stimulation due to elevated levels of beta-human chorionic gonadotropin (beta-hCG) or hypersensitivity to beta-hCG. On ultrasound and MRI, theca lutein cysts appear in multiples on ovaries that are enlarged.

Homeobox protein NOBOX, also known as newborn ovary homeobox protein, is a protein that in humans is encoded by the NOBOX gene. The official symbol (NOBOX) and the official full name are maintained by the HGNC. The NOBOX gene is conserved in chimpanzee, Rhesus monkey, cow, mouse, and rat. There are 175 organisms that have orthologs with human gene NOBOX. It is capable of regulating other genes that are important in the development of follicles. Follicles do not develop and oocytes decrease in its absence which lead to infertility.
Follicle-stimulating hormone (FSH) insensitivity, or ovarian insensitivity to FSH in females, also referable to as ovarian follicle hypoplasia or granulosa cell hypoplasia in females, is a rare autosomal recessive genetic and endocrine syndrome affecting both females and males, with the former presenting with much greater severity of symptomatology. It is characterized by a resistance or complete insensitivity to the effects of follicle-stimulating hormone (FSH), a gonadotropin which is normally responsible for the stimulation of estrogen production by the ovaries in females and maintenance of fertility in both sexes. The condition manifests itself as hypergonadotropic hypogonadism, reduced or absent puberty, amenorrhea, and infertility in females, whereas males present merely with varying degrees of infertility and associated symptoms.
Autoimmunity refers to a pathological immune response of the body's immune system against itself. Autoimmune disease is widely recognized to be significantly more common in women than in men, and often presents differently between the sexes. The reasons for these disparities are still under investigation, but may in part involve the presence of an additional X chromosome in women, as well as the higher presence of female sex hormones such as estrogen. The risk, incidence, and character of autoimmune disease in women may also be associated with female-specific physiological changes, such as hormonal shifts during menses, pregnancy, and menopause.
Ovarian follicle activation can be defined as primordial follicles in the ovary moving from a quiescent (inactive) to a growing phase. The primordial follicle in the ovary is what makes up the “pool” of follicles that will be induced to enter growth and developmental changes that change them into pre-ovulatory follicles, ready to be released during ovulation. The process of development from a primordial follicle to a pre-ovulatory follicle is called folliculogenesis.