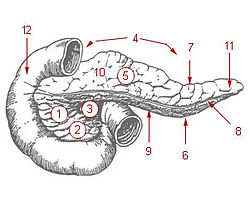
Diagram of the pancreas, showing its relation to the duodenum and the mesenteric veins and arteries
Diagnosis
The diagnosis of this form of injury can be challenging because of the pancreas' location inside the abdomen.[3] The use of ultrasound can reveal fluid around the site of injury.[1]Computed tomography (CT) can also be utilized as a non-invasive diagnostic tool,[3] but its reliability is low; one retrospective case review found that computed tomography had either failed to find injuries or had underestimated the severity of injury in more than half of 17 pancreatic injury patients.[4]Serumamylase has also been shown to be of limited diagnostic utility within the first three hours following injury.[4]
Pancreatic injuries are classified according to the criteria of the American Association for the Surgery of Trauma (AAST). The grade of the trauma should be increased by one level for multiple injuries to the same organ. The description of the injury is that "based on most accurate assessment at autopsy, laparotomy, or radiological study." The pancreatic organ injury scale, as minimally modified, is:[4][6]
When there is no pancreatic duct injury, typically hemostasis and surgical drainage are the main form of treatment.[1][3][4] Surgical repair is undertaken when there is evidence or suspicion of ductal injury.[4] The type of surgery depends on the degree of the injury and its proximity to the mesenteric blood vessels that serve the pancreas. When injuries are not close to the mesenteric vessels, a distal pancreatectomy may be done; this procedure preserves much of the pancreas and usually avoids loss of its endocrine and exocrine functions.[4] In severe cases of pancreaticoduodenal injury, a pancreaticoduodenectomy can be used.[4][7] Common complications after surgery include pancreatitis, pancreatic fistula, abscess, and pseudocyst formation.[2] Initial management of hemorrhage includes controlling it by packing the wound.[5][7]
History
The first recorded case of pancreatic injury was published in The Lancet in 1827.[8] At the time, death as a result of injury was deemed to be "universal".[8] The first successful surgery to repair a transected pancreas was performed in 1904 by Garré, who reported the case the following year.[5][9][10]
↑ "Abstracts of Current Literature". Surgery, Gynecology & Obstetrics. 1. Franklin H. Martin Memorial Foundation, American College of Surgeons: 285. September 1905.
↑ Demetrios Demetriades; Beat Schnüriger; Galinos Barmparas (2010). "49: Pancreatic injury". Surgical Management of Hepatobiliary and Pancreatic Disorders (Seconded.). doi:10.3109/9781841847603. ISBN9781841847603. In 1904, Garre operated successfully on a patient with a transected pancreas.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.