
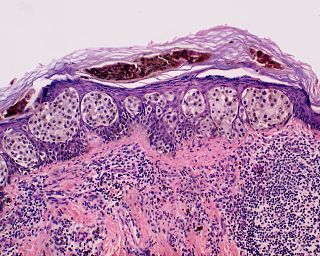
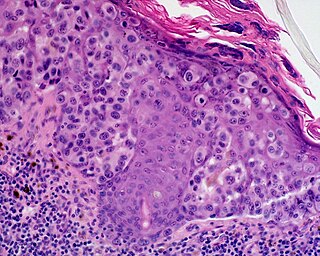
A melanocytic nevus is usually a noncancerous condition of pigment-producing skin cells. It is a type of melanocytic tumor that contains nevus cells. A mole can be either subdermal or a pigmented growth on the skin, formed mostly of a type of cell known as a melanocyte. The high concentration of the body's pigmenting agent, melanin, is responsible for their dark color. Moles are a member of the family of skin lesions known as nevi, occurring commonly in humans. Some sources equate the term "mole" with "melanocytic nevus", but there are also sources that equate the term "mole" with any nevus form.

A biopsy is a medical test commonly performed by a surgeon, an interventional radiologist, or an interventional cardiologist. The process involves the extraction of sample cells or tissues for examination to determine the presence or extent of a disease. The tissue is then fixed, dehydrated, embedded, sectioned, stained and mounted before it is generally examined under a microscope by a pathologist; it may also be analyzed chemically. When an entire lump or suspicious area is removed, the procedure is called an excisional biopsy. An incisional biopsy or core biopsy samples a portion of the abnormal tissue without attempting to remove the entire lesion or tumor. When a sample of tissue or fluid is removed with a needle in such a way that cells are removed without preserving the histological architecture of the tissue cells, the procedure is called a needle aspiration biopsy. Biopsies are most commonly performed for insight into possible cancerous or inflammatory conditions.

Cutaneous squamous-cell carcinoma (cSCC), also known as squamous-cell carcinoma of the skin or squamous-cell skin cancer, is one of the three principal types of skin cancer, alongside basal-cell carcinoma and melanoma. cSCC typically presents as a hard lump with a scaly surface, though it may also present as an ulcer. Onset and development often occurs over several months.
In medicine, Breslow's depth was used as a prognostic factor in melanoma of the skin. It is a description of how deeply tumor cells have invaded. Currently, the standard Breslow's depth has been replaced by the AJCC depth, in the AJCC staging system of melanoma. Originally, Breslow's depth was divided into 5 stages.

Melanoma is the most dangerous type of skin cancer; it develops from the melanin-producing cells known as melanocytes. It typically occurs in the skin, but may rarely occur in the mouth, intestines, or eye.

Nevus is a nonspecific medical term for a visible, circumscribed, chronic lesion of the skin or mucosa. The term originates from nævus, which is Latin for "birthmark"; however, a nevus can be either congenital or acquired. Common terms, including mole, birthmark, and beauty mark, are used to describe nevi, but these terms do not distinguish specific types of nevi from one another.
Superficial spreading melanoma (SSM) is a type of skin cancer that typically starts as an irregularly edged dark spot typically on sun-exposed part of the body. The colour may be variable with dark, light and reddish shades; occasionally no color at all. It typically grows in diameter before spreading to deeper tissue, forming a bump or becoming an ulcer. Itching, bleeding and crust formation may occur in some. The backs and shoulders of males and legs of women are particularly prone.

A dysplastic nevus or atypical mole is a nevus (mole) whose appearance is different from that of common moles. In 1992, the NIH recommended that the term "dysplastic nevus" be avoided in favor of the term "atypical mole". An atypical mole may also be referred to as an atypical melanocytic nevus, atypical nevus, B-K mole, Clark's nevus, dysplastic melanocytic nevus, or nevus with architectural disorder.
Lymph node biopsy is a test in which a lymph node or a piece of a lymph node is removed for examination under a microscope.
Lentigo maligna melanoma is a melanoma that has evolved from a lentigo maligna, as seen as a lentigo maligna with melanoma cells invading below the boundaries of the epidermis. They are usually found on chronically sun damaged skin such as the face and the forearms of the elderly.

Lentigo maligna is where melanocyte cells have become malignant and grow continuously along the stratum basale of the skin, but have not invaded below the epidermis. Lentigo maligna is not the same as lentigo maligna melanoma, as detailed below. It typically progresses very slowly and can remain in a non-invasive form for years.

The congenital melanocytic nevus is a type of melanocytic nevus found in infants at birth. This type of birthmark occurs in an estimated 1% of infants worldwide; it is located in the area of the head and neck 15% of the time.

Mohs surgery, developed in 1938 by a general surgeon, Frederic E. Mohs, is microscopically controlled surgery used to treat both common and rare types of skin cancer. During the surgery, after each removal of tissue and while the patient waits, the tissue is examined for cancer cells. That examination dictates the decision for additional tissue removal. Mohs surgery is the gold standard method for obtaining complete margin control during removal of a skin cancer using frozen section histology. CCPDMA or Mohs surgery allows for the removal of a skin cancer with very narrow surgical margin and a high cure rate.
Surgical pathology is the most significant and time-consuming area of practice for most anatomical pathologists. Surgical pathology involves gross and microscopic examination of surgical specimens, as well as biopsies submitted by surgeons and non-surgeons such as general internists, medical subspecialists, dermatologists, and interventional radiologists.

A blue nevus is a type of coloured mole, typically a single well-defined blue-black bump.

Fibrous papule of the nose is a harmless small bump on or near the nose. It is typically dome-shaped, skin-colored, white or reddish, smooth and firm. Less frequently it can occur elsewhere on the face. Sometimes there are a few. It may be shiny and remains unchanged for life. There may be a central hair.
Pseudomelanoma is a cutaneous condition in which melanotic skin lesions clinically resemble a superficial spreading melanoma at the site of a recent shave removal of a melanocytic nevus.

A pilar sheath acanthoma is a cutaneous condition most often found on the face, particularly above the upper lip in adults. Pilar sheath acanthoma is a skin-colored, 5-10 mm diameter papule or nodule with a keratin-filled pore in the center. Pilar sheath acanthoma diagnosis confirmed by shave or excisional biopsy. Successful treatment requires surgical excision.
Electrodesiccation and curettage is a medical procedure commonly performed by dermatologists, surgeons and general practitioners for the treatment of basal cell cancers and squamous cell cancers of the skin. It provides desiccation, coagulation/cauterization, and curettage to remove lesions from the skin.

A breast biopsy is usually done after a suspicious lesion is discovered on either mammography or ultrasound to get tissue for pathological diagnosis. Several methods for a breast biopsy now exist. The most appropriate method of biopsy for a patient depends upon a variety of factors, including the size, location, appearance and characteristics of the abnormality. The different types of breast biopsies include fine-needle aspiration (FNA), vacuum-assisted biopsy, core needle biopsy, and surgical excision biopsy. Breast biopsies can be done utilizing ultrasound, MRI or a stereotactic biopsy imaging guidance. Vacuum assisted biopsies are typically done using stereotactic techniques when the suspicious lesion can only be seen on mammography. On average, 5–10 biopsies of a suspicious breast lesion will lead to the diagnosis of one case of breast cancer. Needle biopsies have largely replaced open surgical biopsies in the initial assessment of imaging as well as palpable abnormalities in the breast.







