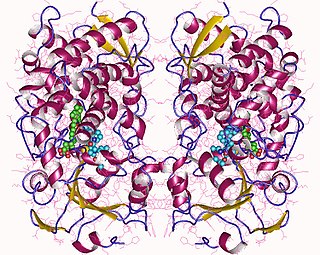
Mechanism of action
The molecular target of the active metabolite of ADP receptor inhibitors is the P2Y12 receptor. [17] P2Y12 receptor is a G-coupled receptor and is activated by adenosine diphosphate. ADP binds to the P2Y12 receptor that leads to inhibition of adenyl cyclase and thereby decreases the intracellular levels of cAMP. This reduction of cAMP reduces phosphorylation of vasodilator stimulated phosphoprotein that leads to the activation of the glycoprotein IIb/IIIa receptors. [18] Activation of the glycoprotein IIb/IIIa receptors increases thromboxane production and prolonged platelet aggregation. [19] Ticlopidine, clopidogrel and prasugrel are thienopyridine prodrugs that are irreversible platelet inhibitors of the P2Y12 receptor. Cangrelor and ticagrelor are direct –acting P2Y12 inhibitors that change the conformation of the P2Y12 receptor and therefore, results in reversible platelet inhibition of the receptor. Thienopyridines are metabolized in the liver and the intestinal to active metabolites. [20]

Metabolism
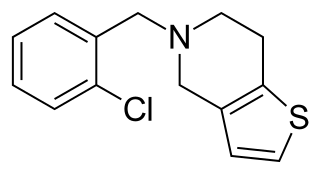
Ticlopidine is a prodrug and is metabolized by at least five main pathways. There is one active metabolite that has been identified and shown to have antiplatelet activity. This active metabolite is formed by a CYP-dependent pathway. CYP2C19 and CYP2B6 are enzymes suggested to contribute to the metabolic transformation of ticlopidine to the thiolactone intermediate, 2-oxo-ticlopidine in the liver. The thiolactone intermediate is then converted to ticlopidine active metabolite via CYP oxidation where oxidation activation occurs. However the CYP enzymes that are involved in this pathway are unknown. [20] In the formation of the active metabolite additional metabolites have been identified and they are dihydrothienopyridinium (M5) and thienodihydropyridinium metabolites (M6). These metabolites may be responsible for the toxic side effects of ticlopidine. [18]

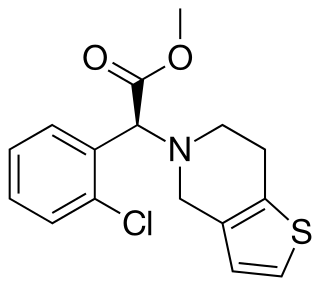
Clopidogrel is a prodrug that is metabolized by two pathways. In one of the pathway most of the dose of clopidogrel (85%) is hydrolyzed by esterases to an inactive carboxylic acid derivate and rapidly cleared via glucoridination followed by renal excretion. The other pathway of clopidogrel requires a two step hepatic CYP450 metabolic activation to produce the active metabolite that inhibits the P2Y12 receptor. CYP1A2, CYP3A4, CYP3A5 and CYP2C19 are considered to be the main enzymes involved in clopidogrel metabolism. [19] First clopidogrel is metabolised into 2-oxo-clopidogrel, which in turn is hydrolyzed to the active metabolism which is a thiol. The thiol forms a disulfide bridge to a cysteine in P2Y12 receptor and thus binds irreversibly to the P2Y12 receptor. Clopidogrel is suggested to bind covalently to CYS17 or CYS270 of the P2Y12 receptor and therefore blocking the binding of the agonist. [18] Some clopidogrel users have defective CYP2C19 activity and therefore poor CYP2C19 metabolism that leads to the risk of reduced activity of clopidogrel. This is because the prodrug does not metabolized to the active drug. Drugs that are CYP2C19 inhibitors can interact with clopidogrel and reduce clopidogrel activity. All proton pump inhibitors except for rabeprazole and pantoprazole are metabolized by the hepatic CYP450 enzyme and therefore, may interact with the metabolism of clopidogrel. Omeprazole is considered to have higher potential for drug-drug interaction than other protein pump inhibitors because it is a CYP2C19 inhibitor. [17]
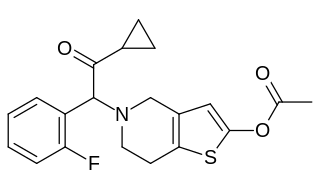
Prasugrel is a third generation thienopyridine and a prodrug. Unlike ticlopidine and clopidogrel, the activation of prasugrel involves hydrolysis to an intermediate thiolactone, which is then converted to the active metabolite in a single CYP-dependent step. The active metabolite, which is R-138727 (thiol intermediate), either binds irreversibly to the P2Y12 receptor or is metabolic methylated to an inactive metabolite. R-138727 is metabolically inactivated via S-methylation. Prasugrel is not metabolized by CYP2C19 like clopidogrel and genetic CYP variants do not have a significant influence on the active metabolites of prasugrel. Prasugrel has more rapid onset of action and greater receptor blocking with the active metabolite than clopidogrel. [18]
Ticagrelor was the first reversible inhibitor of the P2Y12 receptor, active after oral administration. Ticagrelor is orally active without the need for any metabolic activation. It is rapidly absorbed and undergoes enzymatic degradation to at least one active metabolite which is almost as potent as its parent compound. Ticagrelor has improved pharmacokinetic and pharmacodynamic profiles compared to currently available drugs for treating ACS. Moreover, CYP2C19 genotypes that are known to influence the effect of clopidogrel did not influence the effect of ticagrelor. [19]
Cangrelor is the first reversible P2Y12 inhibitor that can by administered intravenously and has a very fast onset and offset, which may provide advantages over current drugs and allow cangrelor to overcome these limitations of oral P2Y12 inhibitor. This makes it an appealing option for antiplatelet therapy, especially for patients who are unable to take oral drugs (e.g. patient who are unconscious, vomiting or sedated). Like ticagrelor it does not require metabolic conversion to be active and therefore it can directly inhibit the P2Y12 receptor. [21]