A lipoma is a benign tumor made of fat tissue. They are generally soft to the touch, movable, and painless. They usually occur just under the skin, but occasionally may be deeper. Most are less than 5 cm (2.0 in) in size. Common locations include upper back, shoulders, and abdomen. It is possible to have a number of lipomas.

Malignancy is the tendency of a medical condition to become progressively worse.

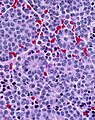
A carcinoid is a slow-growing type of neuroendocrine tumor originating in the cells of the neuroendocrine system. In some cases, metastasis may occur. Carcinoid tumors of the midgut are associated with carcinoid syndrome.
Pleuropulmonary blastoma (PPB) is a rare cancer originating in the lung or pleural cavity. It occurs most often in infants and young children but also has been reported in adults. In a retrospective review of 204 children with lung tumors, pleuropulmonary blastoma and carcinoid tumor were the most common primary tumors. Pleuropulmonary blastoma is regarded as malignant. The male:female ratio is approximately one.

Phyllodes tumors, also cystosarcoma phyllodes, cystosarcoma phylloides and phylloides tumor, are typically large, fast-growing masses that form from the periductal stromal cells of the breast. They account for less than 1% of all breast neoplasms.

Neuroendocrine tumors (NETs) are neoplasms that arise from cells of the endocrine (hormonal) and nervous systems. They most commonly occur in the intestine, where they are often called carcinoid tumors, but they are also found in the pancreas, lung, and the rest of the body.
Appendix cancer are very rare cancers of the vermiform appendix.
Malignant rhabdoid tumour (MRT) is a very aggressive form of tumour originally described as a variant of Wilms' tumour, which is primarily a kidney tumour that occurs mainly in children.

In situ pulmonary adenocarcinoma (AIS)—previously included in the category of "bronchioloalveolar carcinoma" (BAC)—is a subtype of lung adenocarcinoma. It tends to arise in the distal bronchioles or alveoli and is defined by a non-invasive growth pattern. This small solitary tumor exhibits pure alveolar distribution and lacks any invasion of the surrounding normal lung. If completely removed by surgery, the prognosis is excellent with up to 100% 5-year survival.
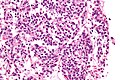
In histopathology, a small-blue-round-cell tumour, also known as a small-round-blue-cell tumor (SRBCT) or a small-round-cell tumour (SRCT), is any one of a group of malignant neoplasms that have a characteristic appearance under the microscope, i.e. consisting of small round cells that stain blue on routine H&E stained sections.

A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.
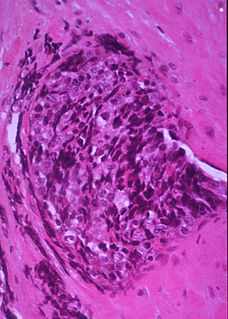
Large cell lung carcinoma with rhabdoid phenotype (LCLC-RP) is a rare histological form of lung cancer, currently classified as a variant of large cell lung carcinoma (LCLC). In order for a LCLC to be subclassified as the rhabdoid phenotype variant, at least 10% of the malignant tumor cells must contain distinctive structures composed of tangled intermediate filaments that displace the cell nucleus outward toward the cell membrane. The whorled eosinophilic inclusions in LCLC-RP cells give it a microscopic resemblance to malignant cells found in rhabdomyosarcoma (RMS), a rare neoplasm arising from transformed skeletal muscle. Despite their microscopic similarities, LCLC-RP is not associated with rhabdomyosarcoma.
Epithelial-myoepithelial carcinoma of the lung is a very rare histologic form of malignant epithelial neoplasm ("carcinoma") arising from lung tissue.
Mucinous cystadenocarcinoma of the lung (MCACL) is a very rare malignant mucus-producing neoplasm arising from the uncontrolled growth of transformed epithelial cells originating in lung tissue.

Giant-cell carcinoma of the lung (GCCL) is a rare histological form of large-cell lung carcinoma, a subtype of undifferentiated lung cancer, traditionally classified within the non-small-cell lung carcinomas (NSCLC).
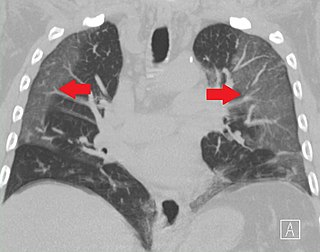
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs. It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process. When a substance other than air fills an area of the lung it increases that area's density. On both x-ray and CT, this appears more grey or hazy as opposed to the normally dark-appearing lungs. Although it can sometimes be seen in normal lungs, common pathologic causes include infections, interstitial lung disease, and pulmonary edema.
Pulmonary carcinoid tumour is a neuroendocrine tumour of the lung.
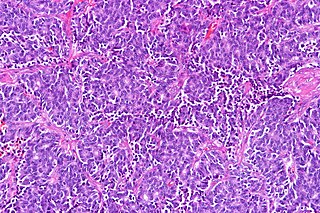
Atypical pulmonary carcinoid tumour is a subtype of pulmonary carcinoid tumor. It is an uncommon low-grade malignant lung mass that is most often in the central airways of the lung. It is also known as "atypical lung carcinoid tumour", " atypical lung carcinoid" or "moderately differentiated neuroendocrine carcinoma".
Pulmonary neuroendocrine tumors are neuroendocrine tumors localized to the lung: bronchus or pulmonary parenchyma.
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) is a diffuse parenchymal lung disease which often presents with symptoms of cough and shortness of breath. The pathological definition published by the World Health Organization is “a generalized proliferation of scattered single cells, small nodules, or linear proliferations of pulmonary neuroendocrine (PNE) cells that may be confined to the bronchial and bronchiolar epithelium.” The true prevalence of this disease is not known. To date, just under 200 cases have been reported in the literature. However, with an increase in recognition of this disease by radiologists and pulmonologists, the number of cases has been increasing. DIPNECH predominantly affects middle-aged women with slowly progressive lung obstruction. DIPNECH is usually discovered in one of two ways: 1) as an unexpected finding following a lung surgery; or 2) by evaluation of a patient in a pulmonary clinic with longstanding, unexplained symptoms.