Related Research Articles
The term abdominal surgery broadly covers surgical procedures that involve opening the abdomen (laparotomy). Surgery of each abdominal organ is dealt with separately in connection with the description of that organ Diseases affecting the abdominal cavity are dealt with generally under their own names.
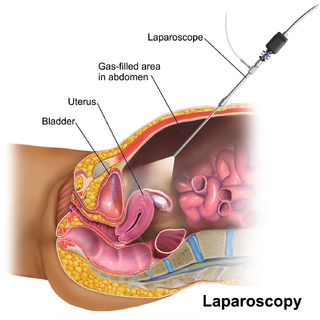
Laparoscopy is an operation performed in the abdomen or pelvis using small incisions with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen.
A hernia is the abnormal exit of tissue or an organ, such as the bowel, through the wall of the cavity in which it normally resides. Various types of hernias can occur, most commonly involving the abdomen, and specifically the groin. Groin hernias are most commonly of the inguinal type but may also be femoral. Other types of hernias include hiatus, incisional, and umbilical hernias. Symptoms are present in about 66% of people with groin hernias. This may include pain or discomfort in the lower abdomen, especially with coughing, exercise, or urinating or defecating. Often, it gets worse throughout the day and improves when lying down. A bulge may appear at the site of hernia, that becomes larger when bending down. Groin hernias occur more often on the right than left side. The main concern is bowel strangulation, where the blood supply to part of the bowel is blocked. This usually produces severe pain and tenderness in the area. Hiatus, or hiatal hernias often result in heartburn but may also cause chest pain or pain while eating.
A hiatal hernia or hiatus hernia is a type of hernia in which abdominal organs slip through the diaphragm into the middle compartment of the chest. This may result in gastroesophageal reflux disease (GERD) or laryngopharyngeal reflux (LPR) with symptoms such as a taste of acid in the back of the mouth or heartburn. Other symptoms may include trouble swallowing and chest pains. Complications may include iron deficiency anemia, volvulus, or bowel obstruction.

Cholecystectomy is the surgical removal of the gallbladder. Cholecystectomy is a common treatment of symptomatic gallstones and other gallbladder conditions. In 2011, cholecystectomy was the eighth most common operating room procedure performed in hospitals in the United States. Cholecystectomy can be performed either laparoscopically, or via an open surgical technique.

Minimally invasive procedures encompass surgical techniques that limit the size of incisions needed, thereby reducing wound healing time, associated pain, and risk of infection. Surgery by definition is invasive and many operations requiring incisions of some size are referred to as open surgery. Incisions made during open surgery can sometimes leave large wounds that may be painful and take a long time to heal. Advancements in medical technologies have enabled the development and regular use of minimally invasive procedures. For example, endovascular aneurysm repair, a minimally invasive surgery, has become the most common method of repairing abdominal aortic aneurysms in the US as of 2003. The procedure involves much smaller incisions than the corresponding open surgery procedure of open aortic surgery.

Hernia repair is a surgical operation for the correction of a hernia—a bulging of internal organs or tissues through the wall that contains it. It can be of two different types: herniorrhaphy; or hernioplasty. This operation may be performed to correct hernias of the abdomen, groin, diaphragm, brain, or at the site of a previous operation. Hernia repair is often performed as an ambulatory procedure.

An umbilical hernia is a health condition where the abdominal wall behind the navel is damaged. It may cause the navel to bulge outwards—the bulge consisting of abdominal fat from the greater omentum or occasionally parts of the small intestine. The bulge can often be pressed back through the hole in the abdominal wall, and may "pop out" when coughing or otherwise acting to increase intra-abdominal pressure. Treatment is surgical, and surgery may be performed for cosmetic as well as health-related reasons.

Perineal hernia is a hernia involving the perineum. The hernia may contain fluid, fat, any part of the intestine, the rectum, or the bladder. It is known to occur in humans, dogs, and other mammals, and often appears as a sudden swelling to one side of the anus.

A Spigelian is the type of ventral hernia where aponeurotic fascia pushes through a hole in the junction of the linea semilunaris and the arcuate line creating a bulge. It appears in the abdomen lower quadrant between an area of dense fibrous tissue and abdominal wall muscles causing a.

A bowel resection or enterectomy is a surgical procedure in which a part of an intestine (bowel) is removed, from either the small intestine or large intestine. Often the word enterectomy is reserved for the sense of small bowel resection, in distinction from colectomy, which covers the sense of large bowel resection. Bowel resection may be performed to treat gastrointestinal cancer, bowel ischemia, necrosis, or obstruction due to scar tissue, volvulus, and hernias. Some patients require ileostomy or colostomy after this procedure as alternative means of excretion. Complications of the procedure may include anastomotic leak or dehiscence, hernias, or adhesions causing partial or complete bowel obstruction. Depending on which part and how much of the intestines are removed, there may be digestive and metabolic challenges afterward, such as short bowel syndrome.
Coccygectomy is a surgical procedure in which the coccyx or tailbone is removed. It is considered a required treatment for sacrococcygeal teratoma and other germ cell tumors arising from the coccyx. Coccygectomy is the treatment of last resort for coccydynia which has failed to respond to nonsurgical treatment. Non surgical treatments include use of seat cushions, external or internal manipulation and massage of the coccyx and the attached muscles, medications given by local injections under fluoroscopic guidance, and medications by mouth.

Diastasis recti, or rectus abdominis diastasis, is defined as a gap of about 2.7 cm or greater between the two sides of the rectus abdominis muscle. The distance between the right and left rectus abdominis muscles is created by the stretching of the linea alba, a connective collagen sheath created by the aponeurosis insertions of the transverse abdominis, internal oblique, and external oblique. This condition has no associated morbidity or mortality. Physical therapy is often required to repair this separation and surgery is an option for more severe cases. Standard exercise rarely results in complete healing of the separated muscles.
Pyloromyotomy is a surgical procedure in which a portion of the muscle fibers of the pyloric muscle are cut. This is typically done in cases where the contents from the stomach are inappropriately stopped by the pyloric muscle, causing the stomach contents to build up in the stomach and unable to be appropriately digested. The procedure is typically performed in cases of "hypertrophic pyloric stenosis" in young children. In most cases, the procedure can be performed with either an open approach or a laparoscopic approach and the patients typically have good outcomes with minimal complications.
Single-port laparoscopy (SPL) is a recently developed technique in laparoscopic surgery. It is a minimally invasive surgical procedure in which the surgeon operates almost exclusively through a single entry point, typically the patient's navel. Unlike a traditional multi-port laparoscopic approach, SPL leaves only a single small scar.
Single-incision laparoscopic surgery (SILS) is an advanced, minimally invasive (keyhole) procedure in which the surgeon operates almost exclusively through a single entry point, typically the patient's umbilicus (navel). Special articulating instruments and access ports eliminate the need to place trochars externally for triangulation, thus allowing the creation of a small, solitary portal of entry into the abdomen.
The Wittmann Patch is a temporary abdominal fascia prosthesis for the planned open abdomen to ease the management of cases where the abdomen cannot be closed due to abdominal compartment syndrome or because multiple further operations are planned. It consists of a sterile hook and a sterile loop sheet made from propylene and nylon.
Inguinal hernia surgery is an operation to repair a weakness in the abdominal wall that abnormally allows abdominal contents to slip into a narrow tube called the inguinal canal in the groin region.
Surgical humidification is the conditioning of insufflation gas with water vapour (humidity) and heat during surgery. Surgical humidification is used to reduce the risk of tissue drying and evaporative cooling.

Surgical mesh is a loosely woven sheet which is used as either a permanent or temporary support for organs and other tissues during surgery. Surgical mesh is created from both inorganic and biological materials and is used in a variety of surgeries. Though hernia repair surgery is the most common application, it can also be used for reconstructive work, such as in pelvic organ prolapse.
References
- ↑ Park, E.; Roth, J.S. (2006). "Abdominal wall hernia". Curr Probl Surg. 43 (5): 326–375. doi:10.1067/j.cpsurg.2006.02.004. PMID 16679124.
- ↑ Bucknall, T.E.; Cox, P.J.; Ellis, H. (1982). "Burst abdomen and incisional hernia: a prospective study of 1129 major laparotomies". Br Med J. 284 (6320): 931–933. doi:10.1136/bmj.284.6320.931. PMC 1496540 . PMID 6279229.
- ↑ Edwards, C.; Geiger, T.; Bartow, K.; et al. (2009). "Laparoscopic transperitoneal repair of flank hernias: A retrospective review of 27 patients". Surg Endosc. 23 (12): 2692–2696. doi:10.1007/s00464-009-0477-4. PMID 19462203. S2CID 22252827.
- ↑ Schumpelick, V.; Klinge, U.; Junge, K.; Stumpf, M. (2004). "Incisional abdominal hernia: the open mesh repair". Langenbecks Arch Surg. 389 (1): 1–5. doi:10.1007/s00423-003-0352-z. PMID 14745557. S2CID 20775829.
- ↑ Lyons, M.; Mohan, H.; Winter, D.C.; Simms, C.K. (2015). "Biomechanical abdominal wall model applied to hernia repair". Br J Surg. 102 (2): e133-139. doi: 10.1002/bjs.9687 . PMID 25627126. S2CID 205514994.
- ↑ Sharma, A.; Dey, A.; Baijal, M.; Chowbey, P.K. (2011). "Laparoscopic repair of suprapubic hernias: transabdominal partial extraperitoneal (TAPE) technique". Surg Endosc. 25 (7): 2147–2152. doi:10.1007/s00464-010-1513-0. PMID 21184109. S2CID 25506589.
- ↑ Matapurkar, B.G.; Bhargave, A.; Dawson, L.; Sonal, B. (1999). "Regeneration of Abdominal Wall Aponeurosis: New Dimension in Marlex Peritoneal Sandwich Repair of Incisional Hernia". World Journal of Surgery. 23 (5): 446–451. doi:10.1007/PL00012326. PMID 10085391. S2CID 22198415.
- ↑ The technique is now published in R. Maingot's textbook of abdominal operations in 1997. [ full citation needed ]
- ↑ Bingener, J.; Buck, L.; Richards, M.; Michalek, J.; Schwesinger, W.; Sirinek, K. (2007). "Long term outcomes in laparoscopic vs open ventral hernia repair". Arch Surg. 142 (6): 562–567. doi: 10.1001/archsurg.142.6.562 . PMID 17576893.
- ↑ Nguyen, S.Q.; Divino, C.M.; Buch, K.E.; Schnur, J.; Weber, K.J.; Katz, L.; Reiner, M.A.; Aldoroty, R.A.; Herron, D.M. (2008). "Postoperative pain after laparoscopic ventral hernia repair: A prospective comparison of sutures versus tacks". Journal of Society of Laparoendoscopic Surgery. 12 (2): 113–116. PMC 3016187 . PMID 18435881.
- ↑ LeBlanc, K.A. (2005). "Incisional hernia repair: Laparoscopic techniques". World Journal of Surgery. 29 (8): 1073–1079. doi:10.1007/s00268-005-7971-1. PMID 15983711. S2CID 189870909.
- ↑ Gurusamy, Kurinchi Selvan; Allen, Victoria B (2013-12-17), The Cochrane Collaboration (ed.), "Wound drains after incisional hernia repair", Cochrane Database of Systematic Reviews, Chichester, UK: John Wiley & Sons, Ltd (12): CD005570.pub4, doi:10.1002/14651858.cd005570.pub4, PMID 24346957