Related Research Articles
Defecation follows digestion, and is a necessary process by which organisms eliminate a solid, semisolid, or liquid waste material known as feces from the digestive tract via the anus or cloaca. The act has a variety of names ranging from the common, like pooping or crapping, to the technical, e.g. bowel movement, to the obscene (shitting), to the euphemistic, to the juvenile. The topic, usually avoided in polite company, can become the basis for some potty humor.

Constipation is a bowel dysfunction that makes bowel movements infrequent or hard to pass. The stool is often hard and dry. Other symptoms may include abdominal pain, bloating, and feeling as if one has not completely passed the bowel movement. Complications from constipation may include hemorrhoids, anal fissure or fecal impaction. The normal frequency of bowel movements in adults is between three per day and three per week. Babies often have three to four bowel movements per day while young children typically have two to three per day.

Fecal incontinence (FI), or in some forms, encopresis, is a lack of control over defecation, leading to involuntary loss of bowel contents, both liquid stool elements and mucus, or solid feces. When this loss includes flatus (gas), it is referred to as anal incontinence. FI is a sign or a symptom, not a diagnosis. Incontinence can result from different causes and might occur with either constipation or diarrhea. Continence is maintained by several interrelated factors, including the anal sampling mechanism, and incontinence usually results from a deficiency of multiple mechanisms. The most common causes are thought to be immediate or delayed damage from childbirth, complications from prior anorectal surgery, altered bowel habits. An estimated 2.2% of community-dwelling adults are affected. However, reported prevalence figures vary. A prevalence of 8.39% among non-institutionalized U.S adults between 2005 and 2010 has been reported, and among institutionalized elders figures come close to 50%.

Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder characterized by a group of symptoms that commonly include abdominal pain, abdominal bloating and changes in the consistency of bowel movements. These symptoms may occur over a long time, sometimes for years. IBS can negatively affect quality of life and may result in missed school or work or reduced productivity at work. Disorders such as anxiety, major depression, and chronic fatigue syndrome are common among people with IBS.

Hirschsprung's disease is a birth defect in which nerves are missing from parts of the intestine. The most prominent symptom is constipation. Other symptoms may include vomiting, abdominal pain, diarrhea and slow growth. Most children develop signs and symptoms shortly after birth. However, others may be diagnosed later in infancy or early childhood. About half of all children with Hirschsprung's disease are diagnosed in the first year of life. Complications may include enterocolitis, megacolon, bowel obstruction and intestinal perforation.
Functional gastrointestinal disorders (FGID), also known as disorders of gut–brain interaction, include a number of separate idiopathic disorders which affect different parts of the gastrointestinal tract and involve visceral hypersensitivity and motility disturbances.
A fecal impaction or an impacted bowel is a solid, immobile bulk of feces that can develop in the rectum as a result of chronic constipation. Fecal impaction is a common result of neurogenic bowel dysfunction and causes immense discomfort and pain. Its treatment includes laxatives, enemas, and pulsed irrigation evacuation (PIE) as well as digital removal. It is not a condition that resolves without direct treatment.
The Bristol stool scale is a diagnostic medical tool designed to classify the form of human faeces into seven categories. It is used in both clinical and experimental fields.

Intestinal pseudo-obstruction (IPO) is a clinical syndrome caused by severe impairment in the ability of the intestines to push food through. It is characterized by the signs and symptoms of intestinal obstruction without any lesion in the intestinal lumen. Clinical features mimic those seen with mechanical intestinal obstructions and can include abdominal pain, nausea, abdominal distension, vomiting, dysphagia and constipation depending upon the part of the gastrointestinal tract involved.
The Rome process and Rome criteria are an international effort to create scientific data to help in the diagnosis and treatment of functional gastrointestinal disorders, such as irritable bowel syndrome, functional dyspepsia and rumination syndrome. The Rome diagnostic criteria are set forth by Rome Foundation, a not for profit 501(c)(3) organization based in Raleigh, North Carolina, United States.

Lubiprostone, sold under the brand name Amitiza among others, is a medication used in the management of chronic idiopathic constipation, predominantly irritable bowel syndrome-associated constipation in women and opioid-induced constipation. The drug is owned by Mallinckrodt and is marketed by Takeda Pharmaceutical Company.
Sacral nerve stimulation, also termed sacral neuromodulation, is a type of medical electrical stimulation therapy.

Prucalopride, sold under brand names Resolor and Motegrity among others, is a medication acting as a selective, high affinity 5-HT4 receptor agonist which targets the impaired motility associated with chronic constipation, thus normalizing bowel movements. Prucalopride was approved for medical use in the European Union in 2009, in Canada in 2011, in Israel in 2014, and in the United States in December 2018. The drug has also been tested for the treatment of chronic intestinal pseudo-obstruction.
Anorectal manometry (ARM) is a medical test used to measure pressures in the anus and rectum and to assess their function. The test is performed by inserting a catheter, that contains a probe embedded with pressure sensors, through the anus and into the rectum. Patients may be asked to perform certain maneuvers, such as coughing or attempting to defecate, to assess for pressure changes. Anorectal manometry is a safe and low risk procedure.
Bile acid malabsorption (BAM), known also as bile acid diarrhea, is a cause of several gut-related problems, the main one being chronic diarrhea. It has also been called bile acid-induced diarrhea, cholerheic or choleretic enteropathy, bile salt diarrhea or bile salt malabsorption. It can result from malabsorption secondary to gastrointestinal disease, or be a primary disorder, associated with excessive bile acid production. Treatment with bile acid sequestrants is often effective. It is recognised as a disability in the United Kingdom under the Equality Act 2010
Solitary rectal ulcer syndrome or SRUS is a chronic, benign disorder of the rectal mucosa. It commonly occurs with varying degrees of rectal prolapse. The condition is thought to be caused by different factors, such as long term constipation, straining during defecation, and dyssynergic defecation. Treatment is by normalization of bowel habits, biofeedback, and other conservative measures. In more severe cases various surgical procedures may be indicated. The condition is relatively rare, affecting approximately 1 in 100,000 people per year. It affects mainly adults aged 30–50. Females are affected slightly more often than males. The disorder can be confused clinically with rectal cancer or other conditions such as inflammatory bowel disease, even when a biopsy is done.
Anismus or dyssynergic defecation is the failure of normal relaxation of pelvic floor muscles during attempted defecation. It can occur in both children and adults, and in both men and women. It can be caused by physical defects or it can occur for other reasons or unknown reasons. Anismus that has a behavioral cause could be viewed as having similarities with parcopresis, or psychogenic fecal retention.
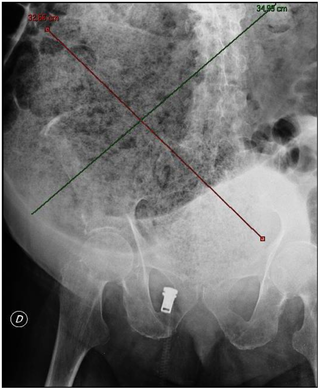
Obstructed defecation syndrome is a major cause of functional constipation, of which it is considered a subtype. It is characterized by difficult and/or incomplete emptying of the rectum with or without an actual reduction in the number of bowel movements per week. Normal definitions of functional constipation include infrequent bowel movements and hard stools. In contrast, ODS may occur with frequent bowel movements and even with soft stools, and the colonic transit time may be normal, but delayed in the rectum and sigmoid colon.
Constipation in children refers to the medical condition of constipation in children. It is a functional gastrointestinal disorder.

Neurogenic bowel dysfunction (NBD) is the inability to control defecation due to a deterioration of or injury to the nervous system, resulting in faecal incontinence or constipation. It is common in people with spinal cord injury (SCI), multiple sclerosis (MS) or spina bifida.
References
- ↑ Shin, Jeong Eun (2022). "Functional Constipation". Sex/Gender-Specific Medicine in the Gastrointestinal Diseases. Singapore: Springer Nature Singapore. p. 259–272. doi:10.1007/978-981-19-0120-1_17. ISBN 978-981-19-0119-5.
- 1 2 "Americal College of Gastroenterology: Fuinctional Bowel Disorders" (PDF). Archived from the original (PDF) on 2011-09-27. Retrieved 2010-06-26.
- ↑ Lacy, Brian E.; Mearin, Fermín; Chang, Lin; Chey, William D.; Lembo, Anthony J.; Simren, Magnus; Spiller, Robin (2016). "Bowel Disorders". Gastroenterology. 150 (6). Elsevier BV: 1393–1407.e5. doi:10.1053/j.gastro.2016.02.031. ISSN 0016-5085.
- ↑ Black, Christopher J; Ford, Alexander C (2018). "Chronic idiopathic constipation in adults: epidemiology, pathophysiology, diagnosis and clinical management". Medical Journal of Australia. 209 (2): 86–91. doi:10.5694/mja18.00241. ISSN 0025-729X.
- ↑ Wald, Ellen R; Di Lorenzo, Carlo; Cipriani, Lynne; Colborn, D Kathleen; Burgers, Rosa; Wald, Arnold (2009). "Bowel Habits and Toilet Training in a Diverse Population of Children". Journal of Pediatric Gastroenterology and Nutrition. 48 (3). Wiley: 294–298. doi:10.1097/mpg.0b013e31817efbf7. ISSN 0277-2116.
- ↑ Burgers, Rosa E.; Mugie, Suzanne M.; Chase, Janet; Cooper, Christopher S.; von Gontard, Alexander; Rittig, Charlotte Siggaard; Homsy, Yves; Bauer, Stuart B.; Benninga, Marc A. (2013). "Management of Functional Constipation in Children with Lower Urinary Tract Symptoms: Report from the Standardization Committee of the International Children's Continence Society". Journal of Urology. 190 (1). Ovid Technologies (Wolters Kluwer Health): 29–36. doi:10.1016/j.juro.2013.01.001. ISSN 0022-5347.
- ↑ Inaloo S, Dehghani SM, Hashemi SM, Heydari M, Heydari ST (2014). "Comorbidity of headache and functional constipation in children: a cross-sectional survey". Turk J Gastroenterol. 25 (5): 508–11. doi:10.5152/tjg.2014.6183. PMID 25417610.
- ↑ Nelson, AD; Camilleri, M; Chirapongsathorn, S; Vijayvargiya, P; Valentin, N; Shin, A; Erwin, PJ; Wang, Z; Murad, MH (September 2017). "Comparison of efficacy of pharmacological treatments for chronic idiopathic constipation: a systematic review and network meta-analysis". Gut. 66 (9): 1611–1622. doi:10.1136/gutjnl-2016-311835. hdl: 1805/12164 . PMID 27287486. S2CID 206964065.
- ↑ Mulhem, E; Khondoker, F; Kandiah, S (1 May 2022). "Constipation in Children and Adolescents: Evaluation and Treatment". American Family Physician. 105 (5): 469–478. PMID 35559625.
- ↑ Ford, Alexander C; Quigley, Eamonn M M; Lacy, Brian E; Lembo, Anthony J; Saito, Yuri A; Schiller, Lawrence R; Soffer, Edy E; Spiegel, Brennan M R; Moayyedi, Paul (2014). "Efficacy of Prebiotics, Probiotics, and Synbiotics in Irritable Bowel Syndrome and Chronic Idiopathic Constipation: Systematic Review and Meta-analysis". The American Journal of Gastroenterology. 109 (10): 1547–1561. doi:10.1038/ajg.2014.202. ISSN 0002-9270. PMID 25070051. S2CID 205100508.
- ↑ Fleisher, DR (November 1976). "Diagnosis and treatment of disorders of defecation in children". Pediatric Annals . 5 (11): 71–101. doi:10.3928/0090-4481-19761101-07. hdl: 10355/5155 . PMID 980548.
- ↑ Firestone Baum, C; John A; Srinivasan K; Harrison P; Kolomensky A; Monagas J; Cocjin J; Hyman PE (January 2013). "Colon manometry proves that perception of the urge to defecate is present in children with functional constipation who deny sensation". Journal of Pediatric Gastroenterology and Nutrition . 56 (1): 19–22. doi: 10.1097/MPG.0b013e31826f2740 . PMID 22922371. S2CID 46075633.