A polyp is an abnormal growth of tissue projecting from a mucous membrane. If it is attached to the surface by a narrow elongated stalk, it is said to be pedunculated; if it is attached without a stalk, it is said to be sessile. Polyps are commonly found in the colon, stomach, nose, ear, sinus(es), urinary bladder, and uterus. They may also occur elsewhere in the body where there are mucous membranes, including the cervix, vocal folds, and small intestine. Some polyps are tumors (neoplasms) and others are non-neoplastic, for example hyperplastic or dysplastic, which are benign. The neoplastic ones are usually benign, although some can be pre-malignant, or concurrent with a malignancy.
The name is of ancient origin, in use in English from about 1400 for a nasal polyp, from Latin polypus through Greek.[1] The animal of similar appearance called polyp is attested from 1742, although the word was earlier used for an octopus.
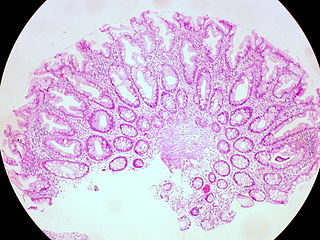
Variable; classical mildly fibrotic polyp with disorganized mucosa and splaying of muscularis mucosae; also inflammatory, juvenile, lipoma, ganglioneuroma, lymphoid
While colon polyps are not commonly associated with symptoms, occasionally they may cause rectal bleeding, and on rare occasions pain, diarrhea or constipation.[9] They are a concern because of the potential for colon cancer being present microscopically, and the risk of benign colon polyps becoming malignant over time.[10] Since most polyps are asymptomatic, they are usually discovered at the time of colon cancer screening. Common screening methods are occult blood test, colonoscopy with a modern flexible endoscope, sigmoidoscopy (usually with the older rigid endoscope), lower gastrointestinal series (barium enema), digital rectal examination (DRE), virtual colonoscopy or Cologuard.[11] The polyps are routinely removed at the time of colonoscopy, either with a wire loop known as a polypectomy snare (first description by P. Deyhle, Germany, 1970),[12] or with biopsy forceps. If an adenomatous polyp is found, it must be removed, since such a polyp is pre-cancerous and has a propensity to become cancerous. For certainty, all polyps which are found by any diagnostic modality, are removed by a colonoscopy. Although colon cancer is usually not found in polyps smaller than 2.5cm, all polyps found are removed since their removal reduces the likelihood of future colon cancer. When adenomatous polyps are removed, a repeat colonoscopy is usually performed three to five years later.[citation needed]
Adenomatous polyps, or adenomas, are polyps that grow on the lining of the colon and which carry a high risk of cancer. The adenomatous polyp is considered pre-malignant, i.e., likely to develop into colon cancer.[14] The other types of polyps that can occur in the colon are hyperplastic and inflammatory polyps, which are unlikely to develop into colorectal cancer.[15]
About 5% of people aged 60 will have at least one adenomatous polyp of 1cm diameter or greater.[16] Multiple adenomatous polyps often result from familial polyposis coli or familial adenomatous polyposis, a condition that carries a very high risk of colon cancer.[13]
Types
Adenomas constitute approximately 10% of digestive polyps. Most polyps (approximately 90%) are small, usually less than 1cm in diameter, and have a small potential for malignancy. The remaining 10% of adenomas are larger than 1cm and approach a 10% chance of containing invasive cancer.[17]
There are three types of adenomatous polyp:
Tubular adenomas (tube-like shape) are the most common of the adenomatous polyps; they may occur everywhere in the colon and they are the least likely colon polyps to develop into colon cancer
Villous adenomas are commonly found in the rectal area and they are normally larger in size than the other two types of adenomas. They tend to be non-pedunculated, velvety, or cauliflower-like in appearance and they are associated with the highest morbidity and mortality rates of all polyps. They can cause hypersecretory syndromes characterized by hypokalemia and profuse mucous discharge, and can harbor carcinoma in situ or invasive carcinoma more frequently than other adenomas.
Risks
The risks of progression to colorectal cancer increase if the polyp is larger than 1cm and contains a higher percentage of villous component. Also, the shape of the polyps is related to the risk of progression into carcinoma. Polyps that are pedunculated (with a stalk) are usually less dangerous than sessile polyps (flat polyps). Sessile polyps have a shorter pathway for migration of invasive cells from the tumor into submucosal and more distant structures, and they are also more difficult to remove and ascertain. Sessile polyps larger than 2cm usually contain villous features, have a higher malignant potential, and tend to recur following colonoscopic polypectomy.[18]
Although polyps do not carry significant risk of colon cancer, tubular adenomatous polyps may become cancerous when they grow larger. Larger tubular adenomatous polyps have an increased risk of malignancy when larger because then they develop more villous components and may become sessile.[19]
It is estimated that an individual whose parents have been diagnosed with an adenomatous polyp has a 50% greater chance to develop colon cancer than individuals with no family history of colonic polyps.[20]As of 2019[update] there is no way to establish the risks of colon polyps of patients with a family history of them. Overall, nearly 6% of the population, regardless of family history, is at risk of developing colon cancer.[citation needed]
Screening
Screening for colonic polyps as well as preventing them has become an important part of the management of the condition. Medical societies have established guidelines for colorectal screening in order to prevent adenomatous polyps and to minimize the chances of developing colon cancer. It is believed that some changes in the diet might be helpful in preventing polyps from occurring, but there is no other way to prevent the polyps from developing into cancerous growths than detecting and removing them.[citation needed]
Colon polyps as they grow can sometimes cause bleeding within the intestine, which can be detected by an occult blood test. According to American Cancer Society guidelines, people over 50 should have an annual occult blood test. People in their 50s are recommended to have flexible sigmoidoscopies performed once every 3 to 5 years to detect any abnormal growth which could be an adenomatous polyp. If adenomatous polyps are detected during this procedure, a colonoscopy is recommended. Medical societies recommend colonoscopies every ten years starting at age 50 as a necessary screening practice for colon cancer.[11][21] The screening provides an accurate image of the intestine and also allows the removal of the polyp, if found. Once an adenomatous polyp is identified during colonoscopy, there are several methods of removal, including using a snare or a heating device.[22] Colonoscopies are preferred over sigmoidoscopies because they allow the examination of the entire colon and can detect polyps in the upper colon, where more than half of polyps occur.[citation needed]
It has been statistically demonstrated that screening programs are effective in reducing the number of deaths caused by colon cancer due to adenomatous polyps. The risk of complications associated with colonoscopies is approximately 0.35 percent, compared to a lifetime risk of developing colon cancer of around 6 percent.[23] As there is a small likelihood of recurrence, surveillance after polyp removal is recommended.[citation needed]
An endometrial polyp or uterine polyp is a polyp or lesion in the lining of the uterus (endometrium) that takes up space within the uterine cavity. Commonly occurring, they are experienced by up to 10% of women.[24] They may have a large flat base (sessile) or be attached to the uterus by an elongated pedicle (pedunculated).[24][25] Pedunculated polyps are more common than sessile ones.[26] They range in size from a few millimeters to several centimeters.[25] If pedunculated, they can protrude through the cervix into the vagina.[24][27] Small blood vessels may be present in polyps, particularly large ones.[24]
A cervical polyp is a common benign polyp or tumor on the surface of the [[Canal of the cervix|cervical canal[28] They can cause irregular menstrual bleeding or increased pain but often show no symptoms.[29]
Polyps on the vocal folds can take on many different forms, and can sometimes result from vocal abuse, although this is not always the cause. They can occur on one or both vocal folds, and appear as swelling, a bump (similar to a nodule), a stalk-like growth, or a blister-like lesion. Most polyps are larger than nodules, which are more similar to callouses on the vocal folds. Polyps and nodules can exhibit similar symptoms including hoarseness or breathiness, "rough" or "scratchy" voice, harshness in vocal quality, shooting pain from ear to ear, sensation of having "a lump in the back of the throat", neck pain, decreased pitch range in the voice, and vocal and bodily fatigue.[citation needed]
If an individual experiences symptoms for more than 2 to 3 weeks, they should see a physician. For a diagnosis, a thorough evaluation of the voice should include a physical examination, preferably by an otolaryngologist (ear, nose, and throat doctor) who specializes in voice, a voice evaluation with a speech-language pathologist (SLP), a neurological examination (in certain cases) The qualities of the voice that will be evaluated include quality, pitch, loudness, and ability to sustain voicing. In some cases, an instrumental examination may be performed with an endoscope into the mouth or nose; this gives a clear look at the vocal folds and larynx in general. In addition to this, a stroboscope (flashing light) may be used to observe the movement of the vocal folds during speech.[citation needed]
Polyps may be treated with medical, surgical, or behavioral intervention. Surgical intervention involves removing the polyp from the vocal fold. This approach is only used when the growth(s) are very large or have existed for an extended amount of time. In children, surgical intervention is rare. Existing medical problems may be treated in an effort to reduce the strain and negative impact on the vocal cords. This could include treatment for gastrointestinal reflux disease, allergies, and thyroid problems. Intervention to stop smoking and reduce stress may also be needed. Most people receive behavioral intervention, or vocal therapy, from an SLP. This might involve teaching good vocal hygiene, and reducing or stopping vocal abuse behaviors. Direct voice treatments may be used to alter pitch, loudness, or breathe support to promote good voicing.[citation needed]
↑ García-Alonso, Francisco Javier; Martín-Mateos, Rosa María; González-Martín, Juan Ángel; Foruny, José Ramón; Vázquez-Sequeiros, Enrique; Boixeda de Miquel, Daniel (2011). "Gastric polyps: analysis of endoscopic and histological features in our center". Revista Española de Enfermedades Digestivas. 103 (8): 416–420. doi:10.4321/S1130-01082011000800005. ISSN1130-0108. PMID21867351.
↑ Naziheh Assarzadegan, M.D., Raul S. Gonzalez, M.D. "Stomach Polyps – Fundic gland polyp". PathologyOutlines.{{cite web}}: CS1 maint: multiple names: authors list (link) Topic Completed: 1 November 2017. Minor changes: 11 December 2019
↑ Varocha Mahachai, MDDavid Y Graham, MDRobert D Odze, MD, FRCPC. "Gastric polyps". UpToDate.{{cite web}}: CS1 maint: multiple names: authors list (link) Literature review current through: Sep 2020. | This topic last updated: Feb 14, 2019.
↑ Fletcher's Diagnostic Histopathology of Tumors, 3rd Ed..
Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum. Signs and symptoms may include blood in the stool, a change in bowel movements, weight loss, abdominal pain and fatigue. Most colorectal cancers are due to old age and lifestyle factors, with only a small number of cases due to underlying genetic disorders. Risk factors include diet, obesity, smoking, and lack of physical activity. Dietary factors that increase the risk include red meat, processed meat, and alcohol. Another risk factor is inflammatory bowel disease, which includes Crohn's disease and ulcerative colitis. Some of the inherited genetic disorders that can cause colorectal cancer include familial adenomatous polyposis and hereditary non-polyposis colon cancer; however, these represent less than 5% of cases. It typically starts as a benign tumor, often in the form of a polyp, which over time becomes cancerous.
Colonoscopy or coloscopy is a medical procedure involving the endoscopic examination of the large bowel (colon) and the distal portion of the small bowel. This examination is performed using either a CCD camera or a fiber optic camera, which is mounted on a flexible tube and passed through the anus.
An adenoma is a benign tumor of epithelial tissue with glandular origin, glandular characteristics, or both. Adenomas can grow from many glandular organs, including the adrenal glands, pituitary gland, thyroid, prostate, and others. Some adenomas grow from epithelial tissue in nonglandular areas but express glandular tissue structure. Although adenomas are benign, they should be treated as pre-cancerous. Over time adenomas may transform to become malignant, at which point they are called adenocarcinomas. Most adenomas do not transform. However, even though benign, they have the potential to cause serious health complications by compressing other structures and by producing large amounts of hormones in an unregulated, non-feedback-dependent manner. Some adenomas are too small to be seen macroscopically but can still cause clinical symptoms.
Gardner's syndrome is a subtype of familial adenomatous polyposis (FAP). Gardner syndrome is an autosomal dominant form of polyposis characterized by the presence of multiple polyps in the colon together with tumors outside the colon. The extracolonic tumors may include osteomas of the skull, thyroid cancer, epidermoid cysts, fibromas, as well as the occurrence of desmoid tumors in approximately 15% of affected individuals.
Familial adenomatous polyposis (FAP) is an autosomal dominant inherited condition in which numerous adenomatous polyps form mainly in the epithelium of the large intestine. While these polyps start out benign, malignant transformation into colon cancer occurs when they are left untreated. Three variants are known to exist, FAP and attenuated FAP are caused by APC gene defects on chromosome 5 while autosomal recessive FAP is caused by defects in the MUTYH gene on chromosome 1. Of the three, FAP itself is the most severe and most common; although for all three, the resulting colonic polyps and cancers are initially confined to the colon wall. Detection and removal before metastasis outside the colon can greatly reduce and in many cases eliminate the spread of cancer.
A benign tumor is a mass of cells (tumor) that does not invade neighboring tissue or metastasize. Compared to malignant (cancerous) tumors, benign tumors generally have a slower growth rate. Benign tumors have relatively well differentiated cells. They are often surrounded by an outer surface or stay contained within the epithelium. Common examples of benign tumors include moles and uterine fibroids.
Gastrointestinal cancer refers to malignant conditions of the gastrointestinal tract and accessory organs of digestion, including the esophagus, stomach, biliary system, pancreas, small intestine, large intestine, rectum and anus. The symptoms relate to the organ affected and can include obstruction, abnormal bleeding or other associated problems. The diagnosis often requires endoscopy, followed by biopsy of suspicious tissue. The treatment depends on the location of the tumor, as well as the type of cancer cell and whether it has invaded other tissues or spread elsewhere. These factors also determine the prognosis.
Fundic gland polyposis is a medical syndrome where the fundus and the body of the stomach develop many fundic gland polyps. The condition has been described both in patients with familial adenomatous polyposis (FAP) and attenuated variants (AFAP), and in patients in whom it occurs sporadically.
Colonic polypectomy is the removal of colorectal polyps in order to prevent them from turning cancerous.
Juvenile polyposis syndrome is an autosomal dominant genetic condition characterized by the appearance of multiple juvenile polyps in the gastrointestinal tract. Polyps are abnormal growths arising from a mucous membrane. These usually begin appearing before age 20, but the term juvenile refers to the type of polyp, not to the age of the affected person. While the majority of the polyps found in juvenile polyposis syndrome are non-neoplastic, hamartomatous, self-limiting and benign, there is an increased risk of adenocarcinoma.
A colorectal polyp is a polyp occurring on the lining of the colon or rectum. Untreated colorectal polyps can develop into colorectal cancer.
Attenuated familial adenomatous polyposis is a form of familial adenomatous polyposis, a cancer syndrome. It is a pre-malignant disease that can develop into colorectal cancer. A patient will have fewer than a hundred polyps located typically in right side of the colon. Cancer might develop as early as the age of five, though typically presents later than classical FAP.
A sessile serrated lesion (SSL) is a premalignant flat lesion of the colon, predominantly seen in the cecum and ascending colon.
A hyperplastic polyp is a type of gastric polyp or colorectal polyp.
The colorectal adenoma is a benign glandular tumor of the colon and the rectum. It is a precursor lesion of the colorectal adenocarcinoma. They often manifest as colorectal polyps.
MUTYH-associated polyposis is an autosomal recessive polyposis syndrome. The disorder is caused by mutations in both alleles of the DNA repair gene, MUTYH. The MUTYH gene encodes a base excision repair protein, which corrects oxidative damage to DNA. Affected individuals have an increased risk of colorectal cancer, precancerous colon polyps (adenomas) and an increased risk of several additional cancers. About 1–2 percent of the population possess a mutated copy of the MUTYH gene, and less than 1 percent of people have the MUTYH-associated polyposis syndrome. The presence of 10 or more colon adenomas should prompt consideration of MUTYH-associated polyposis, familial adenomatous polyposis and similar syndromes.
The histopathology of colorectal cancer of the adenocarcinoma type involves analysis of tissue taken from a biopsy or surgery. A pathology report contains a description of the microscopical characteristics of the tumor tissue, including both tumor cells and how the tumor invades into healthy tissues and finally if the tumor appears to be completely removed. The most common form of colon cancer is adenocarcinoma, constituting between 95% and 98% of all cases of colorectal cancer. Other, rarer types include lymphoma, adenosquamous and squamous cell carcinoma. Some subtypes have been found to be more aggressive.
Serrated polyposis syndrome (SPS), previously known as hyperplastic polyposis syndrome, is a disorder characterized by the appearance of serrated polyps in the colon. While serrated polyposis syndrome does not cause symptoms, the condition is associated with a higher risk of colorectal cancer (CRC). The lifelong risk of CRC is between 25 and 40%. SPS is the most common polyposis syndrome affecting the colon, but is under recognized due to a lack of systemic long term monitoring. Diagnosis requires colonoscopy, and is defined by the presence of either of two criteria: ≥5 serrated lesions/polyps proximal to the rectum, or >20 serrated lesions/polyps of any size distributed throughout the colon with 5 proximal to the rectum.
Polymerase proofreading-associated polyposis (PPAP) is an autosomal dominant hereditary cancer syndrome, which is characterized by numerous polyps in the colon and an increased risk of colorectal cancer. It is caused by germline mutations in DNA polymerase ε (POLE) and δ (POLD1). Affected individuals develop numerous polyps called colorectal adenomas. Compared with other polyposis syndromes, Polymerase proofreading-associated polyposis is rare. Genetic testing can help exclude similar syndromes, such as Familial adenomatous polyposis and MUTYH-associated polyposis. Endometrial cancer, duodenal polyps and duodenal cancer may also occur.
Juvenile polyps are a type of polyp found in the colon. While juvenile polyps are typically found in children, they may be found in people of any age. Juvenile polyps are a type of hamartomatous polyps, which consist of a disorganized mass of tissue. They occur in about two percent of children. Juvenile polyps often do not cause symptoms (asymptomatic); when present, symptoms usually include gastrointestinal bleeding and prolapse through the rectum. Removal of the polyp (polypectomy) is warranted when symptoms are present, for treatment and definite histopathological diagnosis. In the absence of symptoms, removal is not necessary. Recurrence of polyps following removal is relatively common. Juvenile polyps are usually sporadic, occurring in isolation, although they may occur as a part of juvenile polyposis syndrome. Sporadic juvenile polyps may occur in any part of the colon, but are usually found in the distal colon. In contrast to other types of colon polyps, juvenile polyps are not premalignant and are not usually associated with a higher risk of cancer; however, individuals with juvenile polyposis syndrome are at increased risk of gastric and colorectal cancer., Unlike juvenile polyposis syndrome, solitary juvenile polyps do not require follow up with surveillance colonoscopy.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.