
Carpal tunnel syndrome (CTS) is the collection of symptoms and signs associated with nerve compression of the median nerve at the carpal tunnel. Most CTS is related to idiopathic compression of the median nerve as it travels through the wrist at the carpal tunnel. Idiopathic means that there is no other disease process contributing to pressure on the nerve. As with most structural issues, it occurs in both hands, and the strongest risk factor is genetics.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.

Wrist drop is a medical condition in which the wrist and the fingers cannot extend at the metacarpophalangeal joints. The wrist remains partially flexed due to an opposing action of flexor muscles of the forearm. As a result, the extensor muscles in the posterior compartment remain paralyzed.
Peripheral neuropathy, often shortened to neuropathy, is a general term describing damage or disease affecting the nerves. Damage to nerves may impair sensation, movement, gland function, and/or organ function depending on which nerves are affected. Neuropathy affecting motor, sensory, or autonomic nerves result in different symptoms. More than one type of nerve may be affected simultaneously. Peripheral neuropathy may be acute or chronic, and may be reversible or permanent.
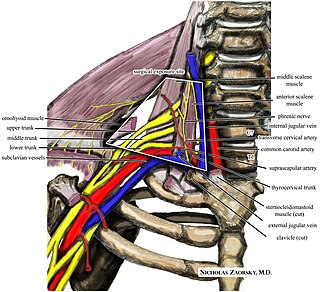
Thoracic outlet syndrome (TOS) is a condition in which there is compression of the nerves, arteries, or veins in the superior thoracic aperture, the passageway from the lower neck to the armpit, also known as the thoracic outlet. There are three main types: neurogenic, venous, and arterial. The neurogenic type is the most common and presents with pain, weakness, paraesthesia, and occasionally loss of muscle at the base of the thumb. The venous type results in swelling, pain, and possibly a bluish coloration of the arm. The arterial type results in pain, coldness, and pallor of the arm.

Polyneuropathy is damage or disease affecting peripheral nerves in roughly the same areas on both sides of the body, featuring weakness, numbness, and burning pain. It usually begins in the hands and feet and may progress to the arms and legs and sometimes to other parts of the body where it may affect the autonomic nervous system. It may be acute or chronic. A number of different disorders may cause polyneuropathy, including diabetes and some types of Guillain–Barré syndrome.
The pronator teres is a muscle that, along with the pronator quadratus, serves to pronate the forearm. It has two origins, at the medial humeral supracondylar ridge and the ulnar tuberosity, and inserts near the middle of the radius.

In the human body, the carpal tunnel or carpal canal is a flattened body cavity on the flexor (palmar/volar) side of the wrist, bounded by the carpal bones and flexor retinaculum. It forms the passageway that transmits the median nerve and the tendons of the extrinsic flexor muscles of the hand from the forearm to the hand. There are described cases of the anatomical variant median artery occurrence.

Ulnar nerve entrapment is a condition where pressure on the ulnar nerve as it passes through the cubital tunnel causes nerve dysfunction (neuropathy). The symptoms of neuropathy are paresthesia (tingling) and numbness primarily affecting the little finger and ring finger of the hand. Ulnar neuropathy can progress to weakness and atrophy of the muscles in the hand. Symptoms can be alleviated by attempts to keep the elbow from flexing while sleeping, such as sticking one's arm in the pillow case, so the pillow restricts flexion.
Ulnar neuropathy is a disorder involving the ulnar nerve. Ulnar neuropathy may be caused by entrapment of the ulnar nerve with resultant numbness and tingling. It may also cause weakness or paralysis of the muscles supplied by the nerve.
Anterior interosseous syndrome is a medical condition in which damage to the anterior interosseous nerve (AIN), a distal motor and sensory branch of the median nerve, classically with severe weakness of the pincer movement of the thumb and index finger, and can cause transient pain in the wrist.
Nerve compression syndrome, or compression neuropathy, or nerve entrapment syndrome, is a medical condition caused by chronic, direct pressure on a peripheral nerve. It is known colloquially as a trapped nerve, though this may also refer to nerve root compression. Its symptoms include pain, tingling, numbness and muscle weakness. The symptoms affect just one particular part of the body, depending on which nerve is affected. The diagnosis is largely clinical and can be confirmed with diagnostic nerve blocks. Occasionally imaging and electrophysiology studies aid in the diagnosis. Timely diagnosis is important as untreated chronic nerve compression may cause permanent damage. A surgical nerve decompression can relieve pressure on the nerve but cannot always reverse the physiological changes that occurred before treatment. Nerve injury by a single episode of physical trauma is in one sense an acute compression neuropathy but is not usually included under this heading, as chronic compression takes a unique pathophysiological course.

A Holstein–Lewis fracture is a fracture of the distal third of the humerus resulting in entrapment of the radial nerve.
Cheiralgia paraesthetica is a neuropathy of the hand generally caused by compression or trauma to the superficial branch of the radial nerve. The area affected is typically on the back or side of the hand at the base of the thumb, near the anatomical snuffbox, but may extend up the back of the thumb and index finger and across the back of the hand. Symptoms include numbness, tingling, burning or pain. Since the nerve branch is sensory there is no motor impairment. It may be distinguished from de Quervain syndrome because it is not dependent on motion of the hand or fingers.
Axillary nerve palsy is a neurological condition in which the axillary nerve has been damaged by shoulder dislocation. It can cause weak deltoid and sensory loss below the shoulder. Since this is a problem with just one nerve, it is a type of Peripheral neuropathy called mononeuropathy. Of all brachial plexus injuries, axillary nerve palsy represents only .3% to 6% of them.
Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.
Crutch paralysis is a form of paralysis which can occur when either the radial nerve or part of the brachial plexus, containing various nerves that innervate sense and motor function to the arm and hand, is under constant pressure, such as by the use of a crutch. This can lead to paralysis of the muscles innervated by the compressed nerve. Generally, crutches that are not adjusted to the correct height can cause the radial nerve to be constantly pushed against the humerus. This can cause any muscle that is innervated by the radial nerve to become partially or fully paralyzed. An example of this is wrist drop, in which the fingers, hand, or wrist is chronically in a flexed position because the radial nerve cannot innervate the extensor muscles due to paralysis. This condition, like other injuries from compressed nerves, normally improves quickly through therapy.
Radial nerve dysfunction is a problem associated with the radial nerve resulting from injury consisting of acute trauma to the radial nerve. The damage has sensory consequences, as it interferes with the radial nerve's innervation of the skin of the posterior forearm, lateral three digits, and the dorsal surface of the lateral side of the palm. The damage also has motor consequences, as it interferes with the radial nerve's innervation of the muscles associated with the extension at the elbow, wrist, and fingers, as well the supination of the forearm. This type of injury can be difficult to localize, but relatively common, as many ordinary occurrences can lead to the injury and resulting mononeuropathy. One out of every ten patients with radial nerve dysfunction do so because of a fractured humerus.
Ischemic monomelic neuropathy(IMN) is an uncommon vascular access complication in hemodialysis patients that manifests as multiple mononeuropathies without clinical ischemia. Ischemic monomelic neuropathy is most likely to affect patients who have had brachiocephalic vascular grafts, and it is characterized by symptoms of acute pain, numbness, and paresthesia in addition to motor weakness. The term "ischemic monomelic neuropathy" was first used in 1983 by Wilbourn, despite the fact that Bolton et al. had originally reported on it in 1979.


