~ 1 in every 10 people,[3][9] 2:1 ratio of men to women, aging and obesity higher risk[5]
Sleep apnea is a sleep-related breathing disorder in which repetitive pauses in breathing, periods of shallow breathing, or collapse of the upper airway during sleep results in poor ventilation and sleep disruption.[10][11] Each pause in breathing can last for a few seconds to a few minutes and occurs many times a night.[1] A choking or snorting sound may occur as breathing resumes.[1] Common symptoms include daytime sleepiness, snoring, and non restorative sleep despite adequate sleep time.[12] Because the disorder disrupts normal sleep, those affected may experience sleepiness or feel tired during the day.[1] It is often a chronic condition.[13]
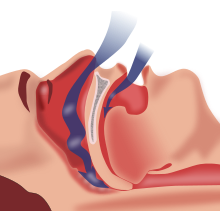
Sleep apnea may be categorized as obstructive sleep apnea (OSA), in which breathing is interrupted by a blockage of air flow, central sleep apnea (CSA), in which regular unconscious breath simply stops, or a combination of the two.[1] OSA is the most common form.[1] OSA has four key contributors; these include a narrow, crowded, or collapsible upper airway, an ineffective pharyngeal dilator muscle function during sleep, airway narrowing during sleep, and unstable control of breathing (high loop gain).[14][15] In CSA, the basic neurological controls for breathing rate malfunction and fail to give the signal to inhale, causing the individual to miss one or more cycles of breathing. If the pause in breathing is long enough, the percentage of oxygen in the circulation can drop to a lower than normal level (hypoxaemia) and the concentration of carbon dioxide can build to a higher than normal level (hypercapnia).[16] In turn, these conditions of hypoxia and hypercapnia will trigger additional effects on the body such as Cheyne-Stokes Respiration.[17]
Some people with sleep apnea are unaware they have the condition.[1] In many cases it is first observed by a family member.[1] An in-lab sleep study overnight is the preferred method for diagnosing sleep apnea.[15] In the case of OSA, the outcome that determines disease severity and guides the treatment plan is the apnea-hypopnea index (AHI).[15] This measurement is calculated from totaling all pauses in breathing and periods of shallow breathing lasting greater than 10 seconds and dividing the sum by total hours of recorded sleep.[10][15] In contrast, for CSA the degree of respiratory effort, measured by esophageal pressure or displacement of the thoracic or abdominal cavity, is an important distinguishing factor between OSA and CSA.[18]
Treatment may include lifestyle changes, mouthpieces, breathing devices, and surgery.[1] Effective lifestyle changes may include avoiding alcohol, losing weight, smoking cessation, and sleeping on one's side.[20] Breathing devices include the use of a CPAP machine.[21] With proper use, CPAP improves outcomes.[22] Evidence suggests that CPAP may improve sensitivity to insulin, blood pressure, and sleepiness.[23][24][25] Long term compliance, however, is an issue with more than half of people not appropriately using the device.[22][26] In 2017, only 15% of potential patients in developed countries used CPAP machines, while in developing countries well under 1% of potential patients used CPAP.[27] Without treatment, sleep apnea may increase the risk of heart attack, stroke, diabetes, heart failure, irregular heartbeat, obesity, and motor vehicle collisions.[1]
OSA is a common sleep disorder. A large analysis in 2019 of the estimated prevalence of OSA found that OSA affects 936 million—1 billion people between the ages of 30–69 globally, or roughly every 1 in 10 people, and up to 30% of the elderly.[28] Sleep apnea is somewhat more common in men than women, roughly a 2:1 ratio of men to women, and in general more people are likely to have it with older age and obesity. Other risk factors include being overweight,[19] a family history of the condition, allergies, and enlarged tonsils.[6]
Signs and symptoms
The typical screening process for sleep apnea involves asking patients about common symptoms such as snoring, witnessed pauses in breathing during sleep and excessive daytime sleepiness.[19] There is a wide range in presenting symptoms in patients with sleep apnea, from being asymptomatic to falling asleep while driving.[19] Due to this wide range in clinical presentation, some people are not aware that they have sleep apnea and are either misdiagnosed or ignore the symptoms altogether.[29] A current area requiring further study involves identifying different subtypes of sleep apnea based on patients who tend to present with different clusters or groupings of particular symptoms.[19]
OSA may increase risk for driving accidents and work-related accidents due to sleep fragmentation from repeated arousals during sleep.[19] If OSA is not treated it results in excessive daytime sleepiness and oxidative stress from the repeated drops in oxygen saturation, people are at increased risk of other systemic health problems, such as diabetes, hypertension or cardiovascular disease.[19] Subtle manifestations of sleep apnea may include treatment refractory hypertension and cardiac arrhythmias and over time as the disease progresses, more obvious symptoms may become apparent.[12] Due to the disruption in daytime cognitive state, behavioral effects may be present. These can include moodiness, belligerence, as well as a decrease in attentiveness and energy.[30] These effects may become intractable, leading to depression.[31]
Risk factors
Obstructive sleep apnea can affect people regardless of sex, race, or age.[32] However, risk factors include:[33]
The causes of obstructive sleep apnea are complex and individualized, but typical risk factors include narrow pharyngeal anatomy and craniofacial structure.[15] When anatomical risk factors are combined with non-anatomical contributors such as an ineffective pharyngeal dilator muscle function during sleep, unstable control of breathing (high loop gain), and premature awakening to mild airway narrowing, the severity of the OSA rapidly increases as more factors are present.[15] When breathing is paused due to upper airway obstruction, carbon dioxide builds up in the bloodstream. Chemoreceptors in the bloodstream note the high carbon dioxide levels. The brain is signaled to awaken the person, which clears the airway and allows breathing to resume. Breathing normally will restore oxygen levels and the person will fall asleep again.[35] This carbon dioxide build-up may be due to the decrease of output of the brainstem regulating the chest wall or pharyngeal muscles, which causes the pharynx to collapse.[36] People with sleep apnea experience reduced or no slow-wave sleep and spend less time in REM sleep.[36]
Central sleep apnea
There are two main mechanism that drive the disease process of CSA, sleep-related hypoventilation and post-hyperventilation hypocapnia.[18] The most common cause of CSA is post-hyperventilation hypocapnia secondary to heart failure.[18] This occurs because of brief failures of the ventilatory control system but normal alveolar ventilation.[18] In contrast, sleep-related hypoventilation occurs when there is a malfunction of the brain's drive to breathe.[18] The underlying cause of the loss of the wakefulness drive to breathe encompasses a broad set of diseases from strokes to severe kyphoscoliosis.[18]
Complications
OSA is a serious medical condition with systemic effects; patients with untreated OSA have a greater mortality risk from cardiovascular disease than those undergoing appropriate treatment.[37] Other complications include hypertension, congestive heart failure, atrial fibrillation, coronary artery disease, stroke, and type 2 diabetes.[37] Daytime fatigue and sleepiness, a common symptom of sleep apnea, is also an important public health concern regarding transportation crashes caused by drowsiness.[37] OSA may also be a risk factor of COVID-19. People with OSA have a higher risk of developing severe complications of COVID-19.[38]
Alzheimer's disease and severe obstructive sleep apnea are connected[39] because there is an increase in the protein beta-amyloid as well as white-matter damage. These are the main indicators of Alzheimer's, which in this case comes from the lack of proper rest or poorer sleep efficiency resulting in neurodegeneration.[3][40][41] Having sleep apnea in mid-life brings a higher likelihood of developing Alzheimer's in older age, and if one has Alzheimer's then one is also more likely to have sleep apnea.[9] This is demonstrated by cases of sleep apnea even being misdiagnosed as dementia.[42] With the use of treatment through CPAP, there is a reversible risk factor in terms of the amyloid proteins. This usually restores brain structure and diminishes cognitive impairment.[43][44][45]
Diagnosis
Classification
There are three types of sleep apnea. OSA accounts for 84%, CSA for 0.9%, and 15% of cases are mixed.[46]
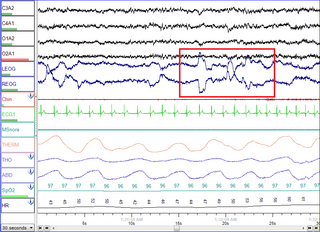
Screenshot of a PSG system showing an obstructive apneaNo airway obstruction during sleepAirway obstruction during sleep
In a systematic review of published evidence, the United States Preventive Services Task Force in 2017 concluded that there was uncertainty about the accuracy or clinical utility of all potential screening tools for OSA,[47] and recommended that evidence is insufficient to assess the balance of benefits and harms of screening for OSA in asymptomatic adults.[48]
The diagnosis of OSA syndrome is made when the patient shows recurrent episodes of partial or complete collapse of the upper airway during sleep resulting in apneas or hypopneas, respectively.[49] Criteria defining an apnea or a hypopnea vary. The American Academy of Sleep Medicine (AASM) defines an apnea as a reduction in airflow of ≥ 90% lasting at least 10 seconds. A hypopnea is defined as a reduction in airflow of ≥ 30% lasting at least 10 seconds and associated with a ≥ 4% decrease in pulse oxygenation, or as a ≥ 30% reduction in airflow lasting at least 10 seconds and associated either with a ≥ 3% decrease in pulse oxygenation or with an arousal.[50]
To define the severity of the condition, the Apnea-Hypopnea Index (AHI) or the Respiratory Disturbance Index (RDI) are used. While the AHI measures the mean number of apneas and hypopneas per hour of sleep, the RDI adds to this measure the respiratory effort-related arousals (RERAs).[51] The OSA syndrome is thus diagnosed if the AHI is > 5 episodes per hour and results in daytime sleepiness and fatigue or when the RDI is ≥ 15 independently of the symptoms.[52] According to the American Association of Sleep Medicine, daytime sleepiness is determined as mild, moderate and severe depending on its impact on social life. Daytime sleepiness can be assessed with the Epworth Sleepiness Scale (ESS), a self-reported questionnaire on the propensity to fall asleep or doze off during daytime.[53] Screening tools for OSA itself comprise the STOP questionnaire, the Berlin questionnaire and the STOP-BANG questionnaire which has been reported as being a very powerful tool to detect OSA.[54][55]
Criteria
According to the International Classification of Sleep Disorders, there are 4 types of criteria. The first one concerns sleep – excessive sleepiness, nonrestorative sleep, fatigue or insomnia symptoms. The second and third criteria are about respiration – waking with breath holding, gasping, or choking; snoring, breathing interruptions or both during sleep. The last criterion revolved around medical issues as hypertension, coronary artery disease, stroke, heart failure, atrial fibrillation, type 2 diabetes mellitus, mood disorder or cognitive impairment. Two levels of severity are distinguished, the first one is determined by a polysomnography or home sleep apnea test demonstrating 5 or more predominantly obstructive respiratory events per hour of sleep and the higher levels are determined by 15 or more events. If the events are present less than 5 times per hour, no obstructive sleep apnea is diagnosed.[56]
A considerable night-to-night variability further complicates diagnosis of OSA. In unclear cases, multiple testing might be required to achieve an accurate diagnosis.[57]
Nighttime in-laboratory Level 1 polysomnography (PSG) is the gold standard test for diagnosis. Patients are monitored with EEG leads, pulse oximetry, temperature and pressure sensors to detect nasal and oral airflow, respiratory impedance plethysmography or similar resistance belts around the chest and abdomen to detect motion, an ECG lead, and EMG sensors to detect muscle contraction in the chin, chest, and legs. A hypopnea can be based on one of two criteria. It can either be a reduction in airflow of at least 30% for more than 10 seconds associated with at least 4% oxygen desaturation or a reduction in airflow of at least 30% for more than 10 seconds associated with at least 3% oxygen desaturation or an arousal from sleep on EEG.[58]
An "event" can be either an apnea, characterized by complete cessation of airflow for at least 10 seconds, or a hypopnea in which airflow decreases by 50 percent for 10 seconds or decreases by 30 percent if there is an associated decrease in the oxygen saturation or an arousal from sleep.[59] To grade the severity of sleep apnea, the number of events per hour is reported as the apnea-hypopnea index (AHI). An AHI of less than 5 is considered normal. An AHI of 5–15 is mild; 15–30 is moderate, and more than 30 events per hour characterizes severe sleep apnea.
Home oximetry
In patients who are at high likelihood of having OSA, a randomized controlled trial found that home oximetry (a non-invasive method of monitoring blood oxygenation) may be adequate and easier to obtain than formal polysomnography.[60] High probability patients were identified by an Epworth Sleepiness Scale (ESS) score of 10 or greater and a Sleep Apnea Clinical Score (SACS) of 15 or greater.[61] Home oximetry, however, does not measure apneic events or respiratory event-related arousals and thus does not produce an AHI value.
The diagnosis of CSA syndrome is made when the presence of at least 5 central apnea events occur per hour.[11] There are multiple mechanisms that drive the apnea events. In individuals with heart failure with Cheyne-Stokes respiration, the brain's respiratory control centers are imbalanced during sleep.[62] This results in ventilatory instability, caused by chemoreceptors that are hyperresponsive to CO2 fluctuations in the blood, resulting in high respiratory drive that leads to apnea.[11] Another common mechanism that causes CSA is the loss of the brain's wakefulness drive to breathe.[11]
Screenshot of a PSG system showing a central apnea
CSA is organized into 6 individual syndromes: Cheyne-Stokes respiration, Complex sleep apnea, Primary CSA, High altitude periodic breathing, CSA from medication, CSA from comorbidity.[11] Like in OSA, nocturnal polysomnography is the mainstay of diagnosis for CSA.[18] The degree of respiratory effort, measured by esophageal pressure or displacement of the thoracic or abdominal cavity, is an important distinguishing factor between OSA and CSA.[18]
Mixed apnea
Some people with sleep apnea have a combination of both types; its prevalence ranges from 0.56% to 18%. The condition, also called treatment-emergent central apnea, is generally detected when obstructive sleep apnea is treated with CPAP and central sleep apnea emerges.[18] The exact mechanism of the loss of central respiratory drive during sleep in OSA is unknown but is most likely related to incorrect settings of the CPAP treatment and other medical conditions the person has.[63]
Management
The treatment of obstructive sleep apnea is different than that of central sleep apnea. Treatment often starts with behavioral therapy and some people may be suggested to try a continuous positive airway pressure device. Many people are told to avoid alcohol, sleeping pills, and other sedatives, which can relax throat muscles, contributing to the collapse of the airway at night.[64] The evidence supporting one treatment option compared to another for a particular person is not clear.[65]
Changing sleep position
More than half of people with obstructive sleep apnea have some degree of positional obstructive sleep apnea, meaning that it gets worse when they sleep on their backs.[66] Sleeping on their sides is an effective and cost-effective treatment for positional obstructive sleep apnea.[66]
Continuous positive airway pressure
Person using a CPAP mask, covering only the noseCPAP device on a nightstand
For moderate to severe sleep apnea, the most common treatment is the use of a continuous positive airway pressure (CPAP) or automatic positive airway pressure (APAP) device.[64][67] These splint the person's airway open during sleep by means of pressurized air. The person typically wears a plastic facial mask, which is connected by a flexible tube to a small bedside CPAP machine.[64]
Although CPAP therapy is effective in reducing apneas and less expensive than other treatments, some people find it uncomfortable. Some complain of feeling trapped, having chest discomfort, and skin or nose irritation. Other side effects may include dry mouth, dry nose, nosebleeds, sore lips and gums.[68]
Whether or not it decreases the risk of death or heart disease is controversial with some reviews finding benefit and others not.[22][69][65] This variation across studies might be driven by low rates of compliance—analyses of those who use CPAP for at least four hours a night suggests a decrease in cardiovascular events.[70]
Weight loss
Excess body weight is thought to be an important cause of sleep apnea.[71] People who are overweight have more tissues in the back of their throat which can restrict the airway, especially when sleeping.[72] In weight loss studies of overweight individuals, those who lose weight show reduced apnea frequencies and improved apnoea–hypopnoea index (AHI).[71][73] Weight loss effective enough to relieve obesity hypoventilation syndrome (OHS) must be 25–30% of body weight. For some obese people, it can be difficult to achieve and maintain this result without bariatric surgery.[74]
In children, orthodontic treatment to expand the volume of the nasal airway, such as nonsurgical rapid palatal expansion is common. The procedure has been found to significantly decrease the AHI and lead to long-term resolution of clinical symptoms.[75][76]
Since the palatal suture is fused in adults, regular RPE using tooth-borne expanders cannot be performed. Mini-implant assisted rapid palatal expansion (MARPE) has been recently developed as a non-surgical option for the transverse expansion of the maxilla in adults. This method increases the volume of the nasal cavity and nasopharynx, leading to increased airflow and reduced respiratory arousals during sleep.[77][78] Changes are permanent with minimal complications.
Surgery
Illustration of surgery on the mouth and throat
Several surgical procedures (sleep surgery) are used to treat sleep apnea, although they are normally a third line of treatment for those who reject or are not helped by CPAP treatment or dental appliances.[22] Surgical treatment for obstructive sleep apnea needs to be individualized to address all anatomical areas of obstruction.[10]
Nasal obstruction
Often, correction of the nasal passages needs to be performed in addition to correction of the oropharynx passage. Septoplasty and turbinate surgery may improve the nasal airway,[79] but has been found to be ineffective at reducing respiratory arousals during sleep.[80]
Uvulopalatopharyngoplasty. A) pre-operative, B) original UPPP, C) modified UPPP, and D) minimal UPPP.
The "Pillar" device is a treatment for snoring and obstructive sleep apnea; it is thin, narrow strips of polyester. Three strips are inserted into the roof of the mouth (the soft palate) using a modified syringe and local anesthetic, in order to stiffen the soft palate. This procedure addresses one of the most common causes of snoring and sleep apnea— vibration or collapse of the soft palate. It was approved by the FDA for snoring in 2002 and for obstructive sleep apnea in 2004. A 2013 meta-analysis found that "the Pillar implant has a moderate effect on snoring and mild-to-moderate obstructive sleep apnea" and that more studies with high level of evidence were needed to arrive at a definite conclusion; it also found that the polyester strips work their way out of the soft palate in about 10% of the people in whom they are implanted.[81]
Hypopharyngeal or base of tongue obstruction
Base-of-tongue advancement by means of advancing the genial tubercle of the mandible, tongue suspension, or hyoid suspension (aka hyoid myotomy and suspension or hyoid advancement) may help with the lower pharynx.[10]
Other surgery options may attempt to shrink or stiffen excess tissue in the mouth or throat, procedures done at either a doctor's office or a hospital. Small shots or other treatments, sometimes in a series, are used for shrinkage, while the insertion of a small piece of stiff plastic is used in the case of surgery whose goal is to stiffen tissues.[64]
Multi-level surgery
Maxillomandibular advancement (MMA) is considered the most effective surgery for people with sleep apnea, because it increases the posterior airway space (PAS).[82] However, health professionals are often unsure as to who should be referred for surgery and when to do so: some factors in referral may include failed use of CPAP or device use; anatomy which favors rather than impedes surgery; or significant craniofacial abnormalities which hinder device use.[83]
Potential complications
Several inpatient and outpatient procedures use sedation. Many drugs and agents used during surgery to relieve pain and to depress consciousness remain in the body at low amounts for hours or even days afterwards. In an individual with either central, obstructive or mixed sleep apnea, these low doses may be enough to cause life-threatening irregularities in breathing or collapses in a patient's airways.[84] Use of analgesics and sedatives in these patients postoperatively should therefore be minimized or avoided.[10]
Surgery on the mouth and throat, as well as dental surgery and procedures, can result in postoperative swelling of the lining of the mouth and other areas that affect the airway. Even when the surgical procedure is designed to improve the airway, such as tonsillectomy and adenoidectomy or tongue reduction, swelling may negate some of the effects in the immediate postoperative period. Once the swelling resolves and the palate becomes tightened by postoperative scarring, however, the full benefit of the surgery may be noticed.[10]
A person with sleep apnea undergoing any medical treatment must make sure their doctor and anesthetist are informed about the sleep apnea. Alternative and emergency procedures may be necessary to maintain the airway of sleep apnea patients.[85]
Other
Neurostimulation
Diaphragm pacing, which involves the rhythmic application of electrical impulses to the diaphragm, has been used to treat central sleep apnea.[86][87]
In April 2014, the U.S. Food and Drug Administration granted pre-market approval for use of an upper airway stimulation system in people who cannot use a continuous positive airway pressure device. The Inspire Upper Airway Stimulation system is a hypoglossal nerve stimulator that senses respiration and applies mild electrical stimulation during inspiration, which pushes the tongue slightly forward to open the airway.[88]
Medications
There is currently insufficient evidence to recommend any medication for OSA.[89] This may result in part because people with sleep apnea have tended to be treated as a single group in clinical trials. Identifying specific physiological factors underlying sleep apnea makes it possible to test drugs specific to those causal factors: airway narrowing, impaired muscle activity, low arousal threshold for waking, and unstable breathing control.[90][91] Those who experience low waking thresholds may benefit from eszopiclone, a sedative typically used to treat insomnia.[90][92] The antidepressant desipramine may stimulate upper airway muscles and lessen pharyngeal collapsibility in people who have limited muscle function in their airways.[90][93]
There is limited evidence for medication, but 2012 AASM guidelines suggested that acetazolamide "may be considered" for the treatment of central sleep apnea; zolpidem and triazolam may also be considered for the treatment of central sleep apnea,[94] but "only if the patient does not have underlying risk factors for respiratory depression".[89][67] Low doses of oxygen are also used as a treatment for hypoxia but are discouraged due to side effects.[95][96][97]
Oral appliances
An oral appliance, often referred to as a mandibular advancement splint, is a custom-made mouthpiece that shifts the lower jaw forward and opens the bite slightly, opening up the airway. These devices can be fabricated by a general dentist. Oral appliance therapy (OAT) is usually successful in patients with mild to moderate obstructive sleep apnea.[98][99] While CPAP is more effective for sleep apnea than oral appliances, oral appliances do improve sleepiness and quality of life and are often better tolerated than CPAP.[99]
Nasal EPAP
Nasal EPAP is a bandage-like device placed over the nostrils that uses a person's own breathing to create positive airway pressure to prevent obstructed breathing.[100]
Oral pressure therapy
Oral pressure therapy uses a device that creates a vacuum in the mouth, pulling the soft palate tissue forward. It has been found useful in about 25 to 37% of people.[101][102]
Prognosis
Death could occur from untreated OSA due to lack of oxygen to the body.[68]
It has been revealed that people with OSA show tissue loss in brain regions that help store memory, thus linking OSA with memory loss.[107] Using magnetic resonance imaging (MRI), the scientists discovered that people with sleep apnea have mammillary bodies that are about 20% smaller, particularly on the left side. One of the key investigators hypothesized that repeated drops in oxygen lead to the brain injury.[108]
The immediate effects of central sleep apnea on the body depend on how long the failure to breathe endures. At worst, central sleep apnea may cause sudden death. Short of death, drops in blood oxygen may trigger seizures, even in the absence of epilepsy. In people with epilepsy, the hypoxia caused by apnea may trigger seizures that had previously been well controlled by medications.[109] In other words, a seizure disorder may become unstable in the presence of sleep apnea. In adults with coronary artery disease, a severe drop in blood oxygen level can cause angina, arrhythmias, or heart attacks (myocardial infarction). Longstanding recurrent episodes of apnea, over months and years, may cause an increase in carbon dioxide levels that can change the pH of the blood enough to cause a respiratory acidosis.[medical citation needed]
The Wisconsin Sleep Cohort Study estimated in 1993 that roughly one in every 15 Americans was affected by at least moderate sleep apnea.[110][111] It also estimated that in middle-age as many as 9% of women and 24% of men were affected, undiagnosed and untreated.[71][110][111]
The costs of untreated sleep apnea reach further than just health issues. It is estimated that in the U.S., the average untreated sleep apnea patient's annual health care costs $1,336 more than an individual without sleep apnea. This may cause $3.4 billion/year in additional medical costs. Whether medical cost savings occur with treatment of sleep apnea remains to be determined.[112]
Frequency and population
Sleep disorders including sleep apnea have become an important health issue in the United States. Twenty-two million Americans have been estimated to have sleep apnea, with 80% of moderate and severe OSA cases undiagnosed.[113]
OSA can occur at any age, but it happens more frequently in men who are over 40 and overweight.[113]
History
A type of CSA was described in the German myth of Ondine's curse where the person when asleep would forget to breathe.[114] The clinical picture of this condition has long been recognized as a character trait, without an understanding of the disease process. The term "Pickwickian syndrome" that is sometimes used for the syndrome was coined by the famous early 20th-century physician William Osler, who must have been a reader of Charles Dickens. The description of Joe, "the fat boy" in Dickens's novel The Pickwick Papers, is an accurate clinical picture of an adult with obstructive sleep apnea syndrome.[115]
The management of obstructive sleep apnea was improved with the introduction of continuous positive airway pressure (CPAP), first described in 1981 by Colin Sullivan and associates in Sydney, Australia.[116] The first models were bulky and noisy, but the design was rapidly improved and by the late 1980s, CPAP was widely adopted. The availability of an effective treatment stimulated an aggressive search for affected individuals and led to the establishment of hundreds of specialized clinics dedicated to the diagnosis and treatment of sleep disorders. Though many types of sleep problems are recognized, the vast majority of patients attending these centers have sleep-disordered breathing. Sleep apnea awareness day is 18 April in recognition of Colin Sullivan.[117]
A sleep disorder, or somnipathy, is a medical disorder of an individual's sleep patterns. Some sleep disorders are severe enough to interfere with normal physical, mental, social and emotional functioning. Sleep disorders are frequent and can have serious consequences on patients' health and quality of life. Polysomnography and actigraphy are tests commonly ordered for diagnosing sleep disorders.
Snoring is the vibration of respiratory structures and the resulting sound due to obstructed air movement during breathing while sleeping. The sound may be soft or loud and unpleasant. Snoring during sleep may be a sign, or first alarm, of obstructive sleep apnea (OSA). Research suggests that snoring is one of the factors of sleep deprivation.
Obesity hypoventilation syndrome (OHS) is a condition in which severely overweight people fail to breathe rapidly or deeply enough, resulting in low oxygen levels and high blood carbon dioxide (CO2) levels. The syndrome is often associated with obstructive sleep apnea (OSA), which causes periods of absent or reduced breathing in sleep, resulting in many partial awakenings during the night and sleepiness during the day. The disease puts strain on the heart, which may lead to heart failure and leg swelling.
Positive airway pressure (PAP) is a mode of respiratory ventilation used in the treatment of sleep apnea. PAP ventilation is also commonly used for those who are critically ill in hospital with respiratory failure, in newborn infants (neonates), and for the prevention and treatment of atelectasis in patients with difficulty taking deep breaths. In these patients, PAP ventilation can prevent the need for tracheal intubation, or allow earlier extubation. Sometimes patients with neuromuscular diseases use this variety of ventilation as well. CPAP is an acronym for "continuous positive airway pressure", which was developed by Dr. George Gregory and colleagues in the neonatal intensive care unit at the University of California, San Francisco. A variation of the PAP system was developed by Professor Colin Sullivan at Royal Prince Alfred Hospital in Sydney, Australia, in 1981.
Upper airway resistance syndrome (UARS) is a sleep disorder characterized by the narrowing of the airway that can cause disruptions to sleep. The symptoms include unrefreshing sleep, fatigue, sleepiness, chronic insomnia, and difficulty concentrating. UARS can be diagnosed by polysomnograms capable of detecting Respiratory Effort-related Arousals. It can be treated with lifestyle changes, functional orthodontics, surgery, mandibular repositioning devices or CPAP therapy. UARS is considered a variant of sleep apnea, although some scientists and doctors believe it to be a distinct disorder.
Polysomnography (PSG), a type of sleep study, is a multi-parameter study of sleep and a diagnostic tool in sleep medicine. The test result is called a polysomnogram, also abbreviated PSG. The name is derived from Greek and Latin roots: the Greek πολύς, the Latin somnus ("sleep"), and the Greek γράφειν.
A mandibi splint or mandibi advancement splint is a prescription custom-made medical device worn in the mouth used to treat sleep-related breathing disorders including: obstructive sleep apnea (OSA), snoring, and TMJ disorders. These devices are also known as mandibular advancement devices, sleep apnea oral appliances, oral airway dilators, and sleep apnea mouth guards.
Non-invasive ventilation (NIV) is the use of breathing support administered through a face mask, nasal mask, or a helmet. Air, usually with added oxygen, is given through the mask under positive pressure; generally the amount of pressure is alternated depending on whether someone is breathing in or out. It is termed "non-invasive" because it is delivered with a mask that is tightly fitted to the face or around the head, but without a need for tracheal intubation. While there are similarities with regard to the interface, NIV is not the same as continuous positive airway pressure (CPAP), which applies a single level of positive airway pressure throughout the whole respiratory cycle; CPAP does not deliver ventilation but is occasionally used in conditions also treated with NIV.
Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder and is characterized by recurrent episodes of complete or partial obstruction of the upper airway leading to reduced or absent breathing during sleep. These episodes are termed "apneas" with complete or near-complete cessation of breathing, or "hypopneas" when the reduction in breathing is partial. In either case, a fall in blood oxygen saturation, a disruption in sleep, or both, may result. A high frequency of apneas or hypopneas during sleep may interfere with the quality of sleep, which – in combination with disturbances in blood oxygenation – is thought to contribute to negative consequences to health and quality of life. The terms obstructive sleep apnea syndrome (OSAS) or obstructive sleep apnea–hypopnea syndrome (OSAHS) may be used to refer to OSA when it is associated with symptoms during the daytime.
Hypopnea is overly shallow breathing or an abnormally low respiratory rate. Hypopnea is defined by some to be less severe than apnea, while other researchers have discovered hypopnea to have a "similar if not indistinguishable impact" on the negative outcomes of sleep breathing disorders. In sleep clinics, obstructive sleep apnea syndrome or obstructive sleep apnea–hypopnea syndrome is normally diagnosed based on the frequent presence of apneas and/or hypopneas rather than differentiating between the two phenomena. Hypopnea is typically defined by a decreased amount of air movement into the lungs and can cause oxygen levels in the blood to drop. It commonly is due to partial obstruction of the upper airway.
Continuous positive airway pressure (CPAP) is a form of positive airway pressure (PAP) ventilation in which a constant level of pressure greater than atmospheric pressure is continuously applied to the upper respiratory tract of a person. The application of positive pressure may be intended to prevent upper airway collapse, as occurs in obstructive sleep apnea, or to reduce the work of breathing in conditions such as acute decompensated heart failure. CPAP therapy is highly effective for managing obstructive sleep apnea. Compliance and acceptance of use of CPAP therapy can be a limiting factor, with 8% of people stopping use after the first night and 50% within the first year.
Sleep medicine is a medical specialty or subspecialty devoted to the diagnosis and therapy of sleep disturbances and disorders. From the middle of the 20th century, research has provided increasing knowledge of, and answered many questions about, sleep–wake functioning. The rapidly evolving field has become a recognized medical subspecialty in some countries. Dental sleep medicine also qualifies for board certification in some countries. Properly organized, minimum 12-month, postgraduate training programs are still being defined in the United States. In some countries, the sleep researchers and the physicians who treat patients may be the same people.
The Apnea–Hypopnea Index or Apnoea–Hypopnoea Index (AHI) is an index used to indicate the severity of sleep apnea. It is represented by the number of apnea and hypopnea events per hour of sleep. Apnea is the complete absence of airflow through your nose and mouth. Hypoapnea is a partial collapse of your airway, limiting breathing. Apneas must last for at least 10 seconds and be associated with a decrease in blood oxygenation to be considered. Combining AHI and oxygen desaturation gives an overall sleep apnea severity score that evaluates both the number of sleep breathing disruptions and the degree of oxygen desaturation during said disruptions.
Catathrenia or nocturnal groaning is a sleep-related breathing disorder, consisting of end-inspiratory apnea and expiratory groaning during sleep. It describes a rare condition characterized by monotonous, irregular groans while sleeping. Catathrenia begins with a deep inspiration. The person with catathrenia holds her or his breath against a closed glottis, similar to the Valsalva maneuver. Expiration can be slow and accompanied by sound caused by vibration of the vocal cords or a simple rapid exhalation. Despite a slower breathing rate, no oxygen desaturation usually occurs. The moaning sound is usually not noticed by the person producing the sound, but it can be extremely disturbing to sleep partners. It appears more often during expiration REM sleep than in NREM sleep.
Christian Guilleminault was a French physician and researcher in the field of sleep medicine who played a central role in the early discovery of obstructive sleep apnea and made seminal discoveries in many other areas of sleep medicine.
Central sleep apnea (CSA) or central sleep apnea syndrome (CSAS) is a sleep-related disorder in which the effort to breathe is diminished or absent, typically for 10 to 30 seconds either intermittently or in cycles, and is usually associated with a reduction in blood oxygen saturation. CSA is usually due to an instability in the body's feedback mechanisms that control respiration. Central sleep apnea can also be an indicator of Arnold–Chiari malformation.
Nasal expiratory positive airway pressure is a treatment for obstructive sleep apnea (OSA) and snoring.
A sleep-related breathing disorder is a sleep disorder in which abnormalities in breathing occur during sleep that may or may not be present while awake. According to the International Classification of Sleep Disorders, sleep-related breathing disorders are classified as follows:
Sleep surgery is a surgery performed to treat sleep disordered breathing. Sleep disordered breathing is a spectrum of disorders that includes snoring, upper airway resistance syndrome, and obstructive sleep apnea. These surgeries are performed by surgeons trained in otolaryngology, oral maxillofacial surgery, and craniofacial surgery.
Oral pressure therapy (OPT) is a treatment for obstructive sleep apnea (OSA) that uses negative pressure in the mouth to shift the soft palate and tongue forward. The negative pressure is created by a bedside console connected by a small tube to a mouthpiece worn inside the mouth during sleep. The device is successful in between a quarter and a third of people.
↑ Haentjens P, Van Meerhaeghe A, Moscariello A, De Weerdt S, Poppe K, Dupont A, Velkeniers B (April 2007). "The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials". Archives of Internal Medicine. 167 (8): 757–64. doi:10.1001/archinte.167.8.757. PMID17452537.
↑ Patel SR, White DP, Malhotra A, Stanchina ML, Ayas NT (March 2003). "Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: results of a meta-analysis". Archives of Internal Medicine. 163 (5): 565–71. doi:10.1001/archinte.163.5.565. PMID12622603.
↑ Berry RB, Quan SF, Abrue AR, et al.; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Version 2.6. Darien, IL: American Academy of Sleep Medicine; 2020.
↑ American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine, 2014.[pageneeded]
↑ Jennifer M. Slowik, Jacob F. Collen (2020). "Obstructive Sleep Apnea". StatPearls. PMID29083619.This article incorporates text available under the CC BY 4.0 license.
↑ Mulgrew AT, Fox N, Ayas NT, Ryan CF (February 2007). "Diagnosis and initial management of obstructive sleep apnea without polysomnography: a randomized validation study". Annals of Internal Medicine. 146 (3): 157–166. doi:10.7326/0003-4819-146-3-200702060-00004. PMID17283346. S2CID25693423.
↑ Flemons WW, Whitelaw WA, Brant R, Remmers JE (November 1994). "Likelihood ratios for a sleep apnea clinical prediction rule". American Journal of Respiratory and Critical Care Medicine. 150 (5 Pt 1): 1279–1285. doi:10.1164/ajrccm.150.5.7952553. PMID7952553.
↑ Yumino D, Bradley TD (February 2008). "Central sleep apnea and Cheyne-Stokes respiration". Proceedings of the American Thoracic Society. 5 (2): 226–36. doi:10.1513/pats.200708-129MG. PMID18250216.
↑ Gottlieb DJ (July 2017). "Does Obstructive Sleep Apnea Treatment Reduce Cardiovascular Risk?: It Is Far Too Soon to Say". JAMA. 318 (2): 128–130. doi:10.1001/jama.2017.7966. PMID28697240.
1 2 3 Young T, Peppard PE, Gottlieb DJ (May 2002). "Epidemiology of Obstructive Sleep Apnea: A Population Health Perspective". American Journal of Respiratory and Critical Care Medicine. 165 (9): 1217–1239. doi:10.1164/rccm.2109080. PMID11991871. S2CID23784058.
↑ Villa MP, Rizzoli A, Miano S, Malagola C (1 May 2011). "Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up". Sleep and Breathing. 15 (2): 179–184. doi:10.1007/s11325-011-0505-1. PMID21437777. S2CID4505051.
↑ Abdullatif J, Certal V, Zaghi S, Song SA, Chang ET, Gillespie MB, Camacho M (1 May 2016). "Maxillary expansion and maxillomandibular expansion for adult OSA: A systematic review and meta-analysis". Journal of Cranio-Maxillofacial Surgery. 44 (5): 574–578. doi:10.1016/j.jcms.2016.02.001. PMID26948172.
↑ Sundaram S, Lim J, Lasserson TJ, Lasserson TJ (19 October 2005). "Surgery for obstructive sleep apnoea in adults". Cochrane Database of Systematic Reviews (4): CD001004. doi:10.1002/14651858.CD001004.pub2. PMID16235277.
↑ Li HY, Wang PC, Chen YP, Lee LA, Fang TJ, Lin HC (January 2011). "Critical Appraisal and Meta-Analysis of Nasal Surgery for Obstructive Sleep Apnea". American Journal of Rhinology & Allergy. 25 (1): 45–49. doi:10.2500/ajra.2011.25.3558. PMID21711978. S2CID35117004.
↑ Choi JH, Kim SN, Cho JH (January 2013). "Efficacy of the Pillar implant in the treatment of snoring and mild-to-moderate obstructive sleep apnea: a meta-analysis". The Laryngoscope. 123 (1): 269–76. doi:10.1002/lary.23470. PMID22865236. S2CID25875843.
↑ Prinsell JR (November 2002). "Maxillomandibular advancement surgery for obstructive sleep apnea syndrome". Journal of the American Dental Association. 133 (11): 1489–97, quiz 1539–40. doi:10.14219/jada.archive.2002.0079. PMID12462692.
↑ MacKay, Stuart (June 2011). "Treatments for snoring in adults". Australian Prescriber. 34 (34): 77–79. doi:10.18773/austprescr.2011.048 (inactive 31 January 2024).{{cite journal}}: CS1 maint: DOI inactive as of January 2024 (link)
↑ "What is Sleep Apnea?". National Heart, Lung, and Blood Institute. National Institutes of Health. 2012. Archived from the original on 28 August 2011. Retrieved 15 February 2013.
1 2 Gaisl T, Haile SR, Thiel S, Osswald M, Kohler M (August 2019). "Efficacy of pharmacotherapy for OSA in adults: A systematic review and network meta-analysis". Sleep Medicine Reviews. 46: 74–86. doi:10.1016/j.smrv.2019.04.009. PMID31075665. S2CID149455430.
↑ Mayos M, Hernández Plaza L, Farré A, Mota S, Sanchis J (January 2001). "Efecto de la oxigenoterapia nocturna en el paciente con síndrome de apnea-hipopnea del sueño y limitación crónica al flujo aéreo" [The effect of nocturnal oxygen therapy in patients with sleep apnea syndrome and chronic airflow limitation]. Archivos de Bronconeumología (in Spanish). 37 (2): 65–68. doi:10.1016/s0300-2896(01)75016-8. PMID11181239.
↑ Breitenbücher A, Keller-Wossidlo H, Keller R (November 1989). "Transtracheale Sauerstofftherapie beim obstruktiven Schlafapnoe-Syndrom" [Transtracheal oxygen therapy in obstructive sleep apnea syndrome]. Schweizerische Medizinische Wochenschrift (in German). 119 (46): 1638–1641. OCLC119157195. PMID2609134.
↑ Machado MA, Juliano L, Taga M, de Carvalho LB, do Prado LB, do Prado GF (December 2007). "Titratable mandibular repositioner appliances for obstructive sleep apnea syndrome: are they an option?". Sleep & Breathing = Schlaf & Atmung. 11 (4): 225–31. doi:10.1007/s11325-007-0109-y. PMID17440760. S2CID24535360.
↑ Kryger MH (December 1985). "Fat, sleep, and Charles Dickens: literary and medical contributions to the understanding of sleep apnea". Clinics in Chest Medicine. 6 (4): 555–62. doi:10.1016/S0272-5231(21)00394-4. PMID3910333.
↑ Sullivan CE, Issa FG, Berthon-Jones M, Eves L (April 1981). "Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares". Lancet. 1 (8225): 862–5. doi:10.1016/S0140-6736(81)92140-1. PMID6112294. S2CID25219388.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.