Related Research Articles
Orthodontics is a dentistry specialty that addresses the diagnosis, prevention, management, and correction of mal-positioned teeth and jaws, as well as misaligned bite patterns. It may also address the modification of facial growth, known as dentofacial orthopedics.

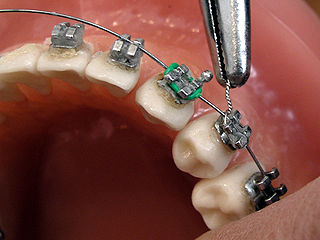
Dental braces are devices used in orthodontics that align and straighten teeth and help position them with regard to a person's bite, while also aiming to improve dental health. They are often used to correct underbites, as well as malocclusions, overbites, open bites, gaps, deep bites, cross bites, crooked teeth, and various other flaws of the teeth and jaw. Braces can be either cosmetic or structural. Dental braces are often used in conjunction with other orthodontic appliances to help widen the palate or jaws and to otherwise assist in shaping the teeth and jaws.
Hypodontia is defined as the developmental absence of one or more teeth excluding the third molars. It is one of the most common dental anomalies, and can have a negative impact on function, and also appearance. It rarely occurs in primary teeth and the most commonly affected are the adult second premolars and the upper lateral incisors. It usually occurs as part of a syndrome that involves other abnormalities and requires multidisciplinary treatment.

In orthodontics, a malocclusion is a misalignment or incorrect relation between the teeth of the upper and lower dental arches when they approach each other as the jaws close. The English-language term dates from 1864; Edward Angle (1855-1930), the "father of modern orthodontics", popularised it. The word "malocclusion" derives from occlusion, and refers to the manner in which opposing teeth meet.

A palatal expander is a device in the field of orthodontics which is used to widen the upper jaw (maxilla) so that the bottom and upper teeth will fit together better. This is a common orthodontic procedure. The use of an expander is most common in children and adolescents 8–18 years of age. It can also be used in adults, although expansion is more uncomfortable and takes longer in adults. A patient who would rather not wait several months for the end result achieved by a palatal expander may be able to opt for a surgical separation of the maxilla. Use of a palatal expander is most often followed by braces to then straighten the teeth.
Orthodontic technology is a specialty of dental technology that is concerned with the design and fabrication of dental appliances for the treatment of malocclusions, which may be a result of tooth irregularity, disproportionate jaw relationships, or both.

Overjet is the extent of horizontal (anterior-posterior) overlap of the maxillary central incisors over the mandibular central incisors. In class II malocclusion the overjet is increased as the maxillary central incisors are protruded.

Crossbite is a form of malocclusion where a tooth has a more buccal or lingual position than its corresponding antagonist tooth in the upper or lower dental arch. In other words, crossbite is a lateral misalignment of the dental arches.
The Damon system of orthodontics is one of many fixed, passive, self-ligating methods of correcting malocclusions. Passive self-ligating systems use brackets that do not require elastic o-rings to hold the wires in place. By not using the elastic o-rings, it is said that the wires freely slide through the slots without friction. However, this may not be correct as it allows more rotation or tipping of teeth before the bracket edges contact the wire, resulting in friction. It is believed that not using o-rings results in better oral hygiene but the research is equivocal, with findings both for and against the theory. To hold the wires in place, the Damon System uses small sliding doors. The addition of 'stops' on the wires helps prevent the wire from becoming displaced from its intended location.

A lingual arch is an orthodontic device which connects two molars in the upper or lower dental arch. The lower lingual arch (LLA) has an archwire adapted to the lingual side of the lower teeth. In the upper arch the archwire is usually connecting the two molars passing through the palatal vault, and is commonly referred as "Transpalatal Arch" (TPA). The TPA was originally described by Robert Goshgarian in 1972. TPAs could possibly be used for maintaining transverse arch widths, anchorage in extraction case, prevent buccal tipping of molars during Burstonian segmented arch mechanics, transverse anchorage and space maintenance.
Self-ligating brackets are defined as "a dental brace, which generally utilizes a permanently installed, moveable component to entrap the archwire". Self-ligating brackets have also been designed which do not require a movable component to hold the wire in place. Self-ligating braces may be classified into two categories: Passive and Active.
Lingual braces are one of the many types of the fixed orthodontic treatment appliances available to patients needing orthodontics. They involve attaching the orthodontic brackets on the inner sides of the teeth. The main advantage of lingual braces is their near invisibility compared to the standard braces, which are attached on the buccal (cheek) sides of the tooth. Lingual braces were invented by Craven Kurz in 1976.
Calvin Suveril Case was an American orthodontist who is one of the earliest figures in orthodontics. Case did extensive work with cleft lip and palate and is known for developing the Velum Obturator. Case is also known for his part in the Extraction Debate of 1911 that happened between Edward Angle and Case.

Anchorage in orthodontics is defined as a way of resisting movement of a tooth or number of teeth by using different techniques. Anchorage is an important consideration in the field of orthodontics as this is a concept that is used frequently when correcting malocclusions. Unplanned or unwanted tooth movement can have dire consequences in a treatment plan, and therefore using anchorage stop a certain tooth movement becomes important. Anchorage can be used from many different sources such as teeth, bone, implants or extra-orally.
Activator Appliance is an Orthodontics appliance that was developed by Viggo Andresen in 1908. This was one of the first functional appliances that was developed to correct functional jaw in the early 1900s. Activator appliance became the universal appliance that was used widely throughout Europe in the earlier part of the 20th century.
Frankel appliance or Frankel Functional Regulator is an orthodontic functional appliance which was developed by Rolf Fränkel in 1950s for treatment to patients of all ages. This appliance primarily focused on the modulation of neuromuscular activity in order to produce changes in jaw and teeth. The appliance was opposite to the Bionator appliance and Activator appliance.
Pendulum is an orthodontic appliance, developed by James J. Hilgers in 1992, that use forces to distalize the upper 1st molars to create space for eruption of impacted teeth or allowing correction of Class 2 malocclusion. This appliance is a fixed type of distalizing appliance that does not depend on the compliance of each patient to work. Hilgers published an article in Journal of Clinical Orthodontics in 1992 describing the appliance.
Intrusion is a movement in the field of orthodontics where a tooth is moved partially into the bone. Intrusion is done in orthodontics to correct an anterior deep bite or in some cases intrusion of the over-erupted posterior teeth with no opposing tooth. Intrusion can be done in many ways and consists of many different types. Intrusion, in orthodontic history, was initially defined as problematic in early 1900s and was known to cause periodontal effects such as root resorption and recession. However, in mid 1950s successful intrusion with light continuous forces was demonstrated. Charles J. Burstone defined intrusion to be "the apical movement of the geometric center of the root (centroid) in respect to the occlusal plane or plane based on the long axis of tooth".
Open bite is a type of orthodontic malocclusion which has been estimated to occur in 0.6% of the people in the United States. This type of malocclusion has no vertical overlap or contact between the anterior incisors. The term "open bite" was coined by Carevelli in 1842 as a distinct classification of malocclusion. Different authors have described the open bite in a variety of ways. Some authors have suggested that open bite often arises when overbite is less than the usual amount. Additionally, others have contended that open bite is identified by end-on incisal relationships. Lastly, some researchers have stated that a lack of incisal contact must be present to diagnose an open bite.
Orthodontic indices are one of the tools that are available for orthodontists to grade and assess malocclusion. Orthodontic indices can be useful for an epidemiologist to analyse prevalence and severity of malocclusion in any population.
References
- 1 2 "Elastics For Braces: Rubber Bands in Orthodontics". Orthodontics Australia. December 15, 2019. Retrieved December 13, 2020.
- ↑ Nolting, Paul R. (August 1, 1937). "Intermaxillary elastics". International Journal of Orthodontia and Oral Surgery. 23 (8): 812–813. doi:10.1016/S1072-3498(37)80050-3.
- ↑ Stewart, C. M.; Chaconas, S. J.; Caputo, A. A. (April 1, 1978). "Effects of intermaxillary elastic traction on orthodontic tooth movement". Journal of Oral Rehabilitation. 5 (2): 159–166. doi:10.1111/j.1365-2842.1978.tb01209.x. ISSN 0305-182X. PMID 280630.
- ↑ "Charles Goodyear | Goodyear Corporate". corporate.goodyear.com. Retrieved September 3, 2016.
- ↑ "Timișoara Medical Journal -The Effect of Intermaxillary Elastics in Orthodontic Therapy". www.tmj.ro. Retrieved September 3, 2016.
- ↑ Janson, Guilherme; Sathler, Renata; Fernandes, Thais Maria Freire; Branco, Nuria Cabral Castello; Freitas, Marcos Roberto de (March 1, 2013). "Correction of Class II malocclusion with Class II elastics: a systematic review". American Journal of Orthodontics and Dentofacial Orthopedics. 143 (3): 383–392. doi:10.1016/j.ajodo.2012.10.015. ISSN 1097-6752. PMID 23452973. S2CID 205354830.
- ↑ Janson, Guilherme; Sathler, Renata; Fernandes, Thais Maria Freire; Branco, Nuria Cabral Castello; de Freitas, Marcos Roberto (March 1, 2013). "Correction of Class II malocclusion with Class II elastics: A 2013 systematic review of 11 studies". American Journal of Orthodontics and Dentofacial Orthopedics. 143 (3): 383–392. doi:10.1016/j.ajodo.2012.10.015. PMID 23452973. S2CID 205354830.
- ↑ Janson, Guilherme; de Freitas, Marcos Roberto; Araki, Janine; Franco, Eduardo Jacomino; Barros, Sérgio Estelita Cavalcante (August 1, 2010). "Class III subdivision malocclusion corrected with asymmetric intermaxillary elastics". American Journal of Orthodontics and Dentofacial Orthopedics. 138 (2): 221–230. doi:10.1016/j.ajodo.2008.08.036. ISSN 1097-6752. PMID 20691365.
- ↑ Zimmer, Bernd; Nischwitz, Diana (September 1, 2012). "Therapeutic changes in the occlusal plane inclination using intermaxillary elastics". Journal of Orofacial Orthopedics. 73 (5): 377–386. doi:10.1007/s00056-012-0100-5. ISSN 1615-6714. PMID 22955576. S2CID 27746651.