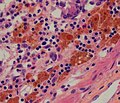
Melanosis coli, also pseudomelanosis coli, is a disorder of pigmentation of the wall of the colon, often identified at the time of colonoscopy. It is benign and may have no significant correlation with disease. The brown pigment is lipofuscin in macrophages, not melanin.[citation needed] It is most commonly associated with the use of certain laxatives.
The most common cause of melanosis coli is the extended use of laxatives, and commonly anthraquinone containing laxatives such as senna, aloe vera, and other plant glycosides.[1] The anthranoid laxatives pass through the gastrointestinal tract unabsorbed until they reach the large intestine, where they are changed into their active forms. The resulting active compounds cause damage to the cells in the lining of the intestine and leads to apoptosis (a form of cell death). The damaged (apoptotic) cells appear as darkly pigmented bodies that may be taken up by scavenger cells known as macrophages. When enough cells have been damaged, the characteristic pigmentation of the bowel wall develops. The condition can develop after just a few months of laxative use.[2]
↑ Byers, R.J.; Marsh, P.; Parkinson, D.; Haboubi, N.Y (October 2003). "Melanosis coli is associated with an increase in colonic epithelial apoptosis and not with laxative use". Histopathology. 30 (2): 160–164. doi:10.1046/j.1365-2559.1997.d01-574.x. PMID9067741. S2CID3175917.
1 2 Wittoesch, JH.; Jackman, RJ.; McDonald, JR. (1958). "Melanosis coli: general review and a study of 887 cases". Dis Colon Rectum. 1 (3): 172–80. doi:10.1007/bf02616828. PMID13537819. S2CID46183745.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.