
The foot is an anatomical structure found in many vertebrates. It is the terminal portion of a limb which bears weight and allows locomotion. In many animals with feet, the foot is a separate organ at the terminal part of the leg made up of one or more segments or bones, generally including claws and/or nails.

Running is a method of terrestrial locomotion by which humans and other animals move rapidly on foot. Running is a gait with an aerial phase in which all feet are above the ground. This is in contrast to walking, where one foot is always in contact with the ground, the legs are kept mostly straight, and the center of gravity vaults over the stance leg or legs in an inverted pendulum fashion. A feature of a running body from the viewpoint of spring-mass mechanics is that changes in kinetic and potential energy within a stride co-occur, with energy storage accomplished by springy tendons and passive muscle elasticity. The term "running" can refer to a variety of speeds ranging from jogging to sprinting.

The leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. The thigh is between the hip and knee, while the calf (rear) and shin (front) are between the knee and foot.

A bunion, also known as hallux valgus, is a deformity of the MTP joint connecting the big toe to the foot. The big toe often bends towards the other toes and the joint becomes red and painful. The onset of bunions is typically gradual. Complications may include bursitis or arthritis.

Pes cavus, also known as high arch, is a human foot type in which the sole of the foot is distinctly hollow when bearing weight. That is, there is a fixed plantar flexion of the foot. A high arch is the opposite of a flat foot and is somewhat less common.

A gait is a manner of limb movements made during locomotion. Human gaits are the various ways in which humans can move, either naturally or as a result of specialized training. Human gait is defined as bipedal forward propulsion of the center of gravity of the human body, in which there are sinuous movements of different segments of the body with little energy spent. Various gaits are characterized by differences in limb movement patterns, overall velocity, forces, kinetic and potential energy cycles, and changes in contact with the ground.

Achilles tendinitis, also known as achilles tendinopathy, occurs when the Achilles tendon, found at the back of the ankle, becomes sore. Achilles tendinopathy is accompanied by alterations in the tendon's structure and mechanical properties. The most common symptoms are pain and swelling around the affected tendon. The pain is typically worse at the start of exercise and decreases thereafter. Stiffness of the ankle may also be present. Onset is generally gradual.

Flat feet, also called pes planus or fallen arches, is a postural deformity in which the arches of the foot collapse, with the entire sole of the foot coming into complete or near-complete contact with the ground. Sometimes children are born with flat feet (congenital). There is a functional relationship between the structure of the arch of the foot and the biomechanics of the lower leg. The arch provides an elastic, springy connection between the forefoot and the hind foot so that a majority of the forces incurred during weight bearing on the foot can be dissipated before the force reaches the long bones of the leg and thigh.
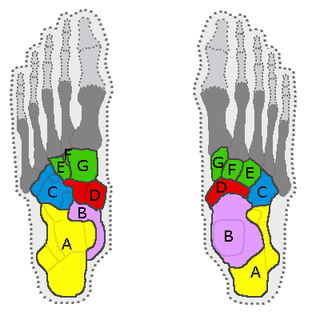
In the human body, the tarsus is a cluster of seven articulating bones in each foot situated between the lower end of the tibia and the fibula of the lower leg and the metatarsus. It is made up of the midfoot and hindfoot.

Foot drop is a gait abnormality in which the dropping of the forefoot happens due to weakness, irritation or damage to the deep fibular nerve, including the sciatic nerve, or paralysis of the muscles in the anterior portion of the lower leg. It is usually a symptom of a greater problem, not a disease in itself. Foot drop is characterized by inability or impaired ability to raise the toes or raise the foot from the ankle (dorsiflexion). Foot drop may be temporary or permanent, depending on the extent of muscle weakness or paralysis and it can occur in one or both feet. In walking, the raised leg is slightly bent at the knee to prevent the foot from dragging along the ground.

Motion, the process of movement, is described using specific anatomical terms. Motion includes movement of organs, joints, limbs, and specific sections of the body. The terminology used describes this motion according to its direction relative to the anatomical position of the body parts involved. Anatomists and others use a unified set of terms to describe most of the movements, although other, more specialized terms are necessary for describing unique movements such as those of the hands, feet, and eyes.

Barefoot running, also called "natural running", is the act of running without footwear. With the advent of modern footwear, running barefoot has become less common in most parts of the world but is still practiced in parts of Africa and Latin America. In some Western countries, barefoot running has grown in popularity due to perceived health benefits.
The Ponseti method is a manipulative technique that corrects congenital clubfoot without invasive surgery. It was developed by Ignacio V. Ponseti of the University of Iowa Hospitals and Clinics, US, in the 1950s, and was repopularized in 2000 by John Herzenberg in the US and Europe and in Africa by NHS surgeon Steve Mannion. It is a standard treatment for clubfoot.
Cuboid syndrome or cuboid subluxation describes a condition that results from subtle injury to the calcaneocuboid joint and ligaments in the vicinity of the cuboid bone, one of seven tarsal bones of the human foot.

Comparative foot morphology involves comparing the form of distal limb structures of a variety of terrestrial vertebrates. Understanding the role that the foot plays for each type of organism must take account of the differences in body type, foot shape, arrangement of structures, loading conditions and other variables. However, similarities also exist among the feet of many different terrestrial vertebrates. The paw of the dog, the hoof of the horse, the manus (forefoot) and pes (hindfoot) of the elephant, and the foot of the human all share some common features of structure, organization and function. Their foot structures function as the load-transmission platform which is essential to balance, standing and types of locomotion.

Orthotics is a medical specialty that focuses on the design and application of orthoses, sometimes known as braces or calipers. An orthosis is "an externally applied device used to influence the structural and functional characteristics of the neuromuscular and skeletal systems." Orthotists are professionals who specialize in designing these braces.

Locomotor effects of shoes are the way in which the physical characteristics or components of shoes influence the locomotion neuromechanics of a person. Depending on the characteristics of the shoes, the effects are various, ranging from alteration in balance and posture, muscle activity of different muscles as measured by electromyography (EMG), and the impact force. There are many different types of shoes that exist, such as running, walking, loafers, high heels, sandals, slippers, work boots, dress shoes, and many more. However, a typical shoe will be composed of an insole, midsole, outsole, and heels, if any. In an unshod condition, where one is without any shoes, the locomotor effects are primarily observed in the heel strike patterns and resulting impact forces generated on the ground.
Children's feet are smaller than those of adults, not reaching full size until the ages of 13 in girls and 15 in boys. There are correspondingly small sizes of shoes for them. In poor populations and tropical countries, children commonly go barefoot.
Running injuries affect about half of runners annually. The frequencies of various RRI depend on the type of running, such as speed and mileage. Some injuries are acute, caused by sudden overstress, such as side stitch, strains, and sprains. Many of the common injuries that affect runners are chronic, developing over longer periods as the result of overuse. Common overuse injuries include shin splints, stress fractures, Achilles tendinitis, Iliotibial band syndrome, Patellofemoral pain, and plantar fasciitis.



