
Cervical cancer is a cancer arising from the cervix or in the any layer of the wall of the cervix. It is due to the abnormal growth of cells that have the ability to invade or spread to other parts of the body. Early on, typically no symptoms are seen. Later symptoms may include abnormal vaginal bleeding, pelvic pain or pain during sexual intercourse. While bleeding after sex may not be serious, it may also indicate the presence of cervical cancer.

Hysterectomy is the surgical removal of the uterus and cervix. Supracervical hysterectomy refers to removal of the uterus while the cervix is spared. These procedures may also involve removal of the ovaries (oophorectomy), fallopian tubes (salpingectomy), and other surrounding structures. The term “partial” or “total” hysterectomy are lay-terms that incorrectly describe the addition or omission of oophorectomy at the time of hysterectomy. These procedures are usually performed by a gynecologist. Removal of the uterus renders the patient unable to bear children and has surgical risks as well as long-term effects, so the surgery is normally recommended only when other treatment options are not available or have failed. It is the second most commonly performed gynecological surgical procedure, after cesarean section, in the United States. Nearly 68 percent were performed for conditions such as endometriosis, irregular bleeding, and uterine fibroids. It is expected that the frequency of hysterectomies for non-malignant indications will continue to fall given the development of alternative treatment options.

Endometrial cancer is a cancer that arises from the endometrium. It is the result of the abnormal growth of cells that have the ability to invade or spread to other parts of the body. The first sign is most often vaginal bleeding not associated with a menstrual period. Other symptoms include pain with urination, pain during sexual intercourse, or pelvic pain. Endometrial cancer occurs most commonly after menopause.

Cervical intraepithelial neoplasia (CIN), also known as cervical dysplasia, is the abnormal growth of cells on the surface of the cervix that could potentially lead to cervical cancer. More specifically, CIN refers to the potentially precancerous transformation of cells of the cervix.

Vaginectomy is a surgery to remove all or part of the vagina. It is one form of treatment for individuals with vaginal cancer or rectal cancer that is used to remove tissue with cancerous cells. It can also be used in gender-affirming surgery. Some people born with a vagina who identify as trans men or as nonbinary may choose vaginectomy in conjunction with other surgeries to make the clitoris more penis-like (metoidioplasty), construct of a full-size penis (phalloplasty), or create a relatively smooth, featureless genital area.

Primary peritoneal cancer or carcinoma is also known as serous surface papillary carcinoma, primary peritoneal carcinoma, extra-ovarian serous carcinoma, primary serous papillary carcinoma, and psammomacarcinoma. It was historically classified under "carcinoma of unknown primary" (CUP). Primary peritoneal cancer is a cancer of the cells lining the peritoneum, or abdominal cavity. It usually affects women and is diagnosed after the age of 60; it very rarely affects men.

The cardinal ligament is a major ligament of the uterus formed as a thickening of connective tissue of the base of the broad ligament of the uterus. It extends laterally from the cervix and vaginal fornix to attach onto the lateral wall of the pelvis. The female ureter, uterine artery, and inferior hypogastric (nervous) plexus course within the cardinal ligament. The cardinal ligament supports the uterus.
Gynecologic oncology is a specialized field of medicine that focuses on cancers of the female reproductive system, including ovarian cancer, uterine cancer, vaginal cancer, cervical cancer, and vulvar cancer. As specialists, they have extensive training in the diagnosis and treatment of these cancers.
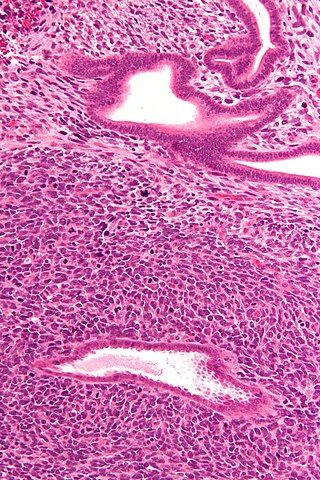
Sarcoma botryoides or botryoid sarcoma is a subtype of embryonal rhabdomyosarcoma, that can be observed in the walls of hollow, mucosa lined structures such as the nasopharynx, common bile duct, urinary bladder of infants and young children or the vagina in females, typically younger than age 8. The name comes from the gross appearance of "grape bunches".
Gynecologic cancer is a type of cancer that affects the female reproductive system, including ovarian cancer, uterine cancer, vaginal cancer, cervical cancer, and vulvar cancer.

Primary fallopian tube cancer (PFTC), also known as tubal cancer, is a malignant neoplasm that originates from the fallopian tube. Along with primary ovarian and peritoneal carcinomas, it is grouped under epithelial ovarian cancers; cancers of the ovary that originate from a fallopian tube precursor.

Uterine serous carcinoma is a malignant form of serous tumor that originates in the uterus. It is an uncommon form of endometrial cancer that typically arises in postmenopausal women. It is typically diagnosed on endometrial biopsy, prompted by post-menopausal bleeding.
Neuroendocrine carcinoma of the cervix is best defined separately:Neuroendocrine: Of, relating to, or involving the interaction between the nervous system and the hormones of the endocrine glands.Carcinoma: An invasive malignant tumor derived from epithelial tissue that tends to metastasize to other areas of the body.

A cervical pregnancy is an ectopic pregnancy that has implanted in the uterine endocervix. Such a pregnancy typically aborts within the first trimester, however, if it is implanted closer to the uterine cavity – a so-called cervico-isthmic pregnancy – it may continue longer. Placental removal in a cervical pregnancy may result in major hemorrhage.

Clear-cell adenocarcinoma is a rare and aggressive form of cancer that typically arises in the female reproductive organs, particularly the ovaries and the endometrium as well as the kidneys and is characterized by the presence of clear, glycogen-rich cells. Specific criteria must be met for a tumor to be classified as clear cell adenocarcinoma. According to the WHO, these criteria include polygonal or hobnail or cells with clear or eosinophilic/oxyphilic cytoplasm and nuclear atypia, with different architectural patterns of growth, such as papillary, tubulocystic, or solid.
Uterine adenosarcoma is an uncommon form of cancer that arises from mesenchymal tissue of the uterus and has a benign glandular component.
A lymphocele is a collection of lymphatic fluid within the body not bordered by epithelial lining. It is usually a surgical complication seen after extensive pelvic surgery and is most commonly found in the retroperitoneal space. Spontaneous development is rare.

The Wertheim–Meigs operation is a surgical procedure for the treatment of cervical cancer performed by way of an abdominal incision.

William Francis Victor Bonney FRCP FRCS was a prominent British gynaecological surgeon. He was described by Geoffrey Chamberlain as "a primary influence on world gynaecology in the years between the wars".
Bradley J. Monk is an American gynecologic oncologist, academician and researcher. He is a professor on the Clinical Scholar Track in the Department of Obstetrics and Gynecology at the University of Arizona College of Medicine in Phoenix, Arizona, as well as at the Creighton University School of Medicine in Omaha, Nebraska. He also serves as Director of the Division of Gynecologic Oncology at the St. Joseph's Hospital and Medical Center in Phoenix.
