In obstetrics, gestational age is a measure of the age of a pregnancy taken from the beginning of the woman's last menstrual period (LMP),[1] or the corresponding age of the gestation as estimated by a more accurate method, if available. Such methods include adding 14 days to a known duration since fertilization (as is possible in in vitro fertilization), or by obstetric ultrasonography. The popularity of using this measure of pregnancy is largely due to convenience: menstruation is usually noticed, while there is generally no convenient way to discern when fertilization or implantation occurred.
Directly calculating the days since the beginning of the last menstrual period
Early obstetric ultrasound, comparing the size of an embryo or fetus to that of a reference group of pregnancies of known gestational age (such as calculated from last menstrual periods) and using the mean gestational age of other embryos or fetuses of the same size. If the gestational age as calculated from an early ultrasound is contradictory to the one calculated directly from the last menstrual period, it is still the one from the early ultrasound that is used for the rest of the pregnancy.[2]
Gestational age can also be estimated by calculating days from ovulation if it was estimated from related signs or ovulation tests, and adding 14 days by convention.[4]
A more complete listing of methods is given in following table:[5]
As a general rule, the official gestational age should be based on the actual beginning of the last menstrual period, unless any of the above methods gives an estimated date that differs more than the variability for the method, in which case the difference cannot probably be explained by that variability alone.[5] For example, if there is a gestational age based on the beginning of the last menstrual period of 9.0 weeks, and a first-trimester obstetric ultrasonography gives an estimated gestational age of 10.0 weeks (with a 2 SD variability of ±8% of the estimate, thereby giving a variability of ±0.8 weeks), the difference of 1.0 weeks between the tests is larger than the 2 SD variability of the ultrasonography estimate, indicating that the gestational age estimated by ultrasonography should be used as the official gestational age.[5]
Once the estimated due date (EDD) is established, it should rarely be changed, as the determination of gestational age is most accurate earlier in the pregnancy.[6]
Assessment of gestational age can be made based on selected head and trunk parameters.[7] Following are diagrams for estimating gestational age from obstetric ultrasound, by various target parameters:
The fertilization or conceptional age (also called embryonic age and later fetal age) is the time from the fertilization. It usually occurs within a day of ovulation, which, in turn, occurs on average 14.6 days after the beginning of the preceding menstruation (LMP).[8]
There is also considerable variability in this interval, with a 95% prediction interval of the ovulation of 9 to 20 days after menstruation even for an average woman who has a mean LMP-to-ovulation time of 14.6.[9] In a reference group representing all women, the 95% prediction interval of the LMP-to-ovulation is 8.2 to 20.5 days.[8] The actual variability between gestational age as estimated from the beginning of the last menstrual period (without the use of any additional method mentioned in previous section) is substantially larger because of uncertainty which menstrual cycle gave rise to the pregnancy. For example, the menstruation may be scarce enough to give the false appearance that an earlier menstruation gave rise to the pregnancy, potentially giving an estimated gestational age that is approximately one month too large. Also, vaginal bleeding occurs during 15–25% of first trimester pregnancies,[10] and may be mistaken as menstruation, potentially giving an estimated gestational age that is too low.
Comparison of dating systems for a typical pregnancy
Distribution of gestational age at childbirth among singleton live births, given both when gestational age is estimated by first trimester ultrasound and directly by last menstrual period
The mean pregnancy length has been estimated to be 283.4 days of gestational age as timed from the first day of the last menstrual period and 280.6 days when retrospectively estimated by obstetric ultrasound measurement of the fetal biparietal diameter (BPD) in the second trimester.[14] Other algorithms take into account other variables, such as whether this is the first or subsequent child, the mother's race, age, length of menstrual cycle, and menstrual regularity. In order to have a standard reference point, the normal pregnancy duration is assumed by medical professionals to be 280 days (or 40 weeks) of gestational age. Furthermore, actual childbirth has only a certain probability of occurring within the limits of the estimated due date. A study of singleton live births determined that childbirth has a standard deviation of 14 days when gestational age is estimated by first-trimester ultrasound and 16 days when estimated directly by last menstrual period.[13]
The most common system used among healthcare professionals is Naegele's rule, which estimates the expected date of delivery (EDD) by adding a year, subtracting three months, and adding seven days to the first day of a woman's last menstrual period (LMP) or corresponding date as estimated from other means.
Medical fetal viability
There is no sharp limit of development, gestational age, or weight at which a human fetus automatically becomes viable.[15] According to studies between 2003 and 2005, 20 to 35 percent of babies born at 23 weeks of gestation survive, while 50 to 70 percent of babies born at 24 to 25 weeks, and more than 90 percent born at 26 to 27 weeks, survive.[16] It is rare for a baby weighing less than 500g (17.6ounces) to survive.[15] A baby's chances for survival increases 3–4% per day between 23 and 24 weeks of gestation and about 2–3% per day between 24 and 26 weeks of gestation. After 26 weeks the rate of survival increases at a much slower rate because survival is high already.[17] Prognosis depends also on medical protocols on whether to resuscitate and aggressively treat a very premature newborn, or whether to provide only palliative care, in view of the high risk of severe disability of very preterm babies.[18]
Stages in prenatal development, showing viability and point of 50% chance of survival (limit of viability) at bottom. Weeks and months numbered by gestation.
Using the LMP (last menstrual period) method, a full-term human pregnancy is considered to be 40 weeks (280 days), though pregnancy lengths between 38 and 42 weeks are considered normal. A fetus born prior to the 37th week of gestation is considered to be preterm. A preterm baby is likely to be premature and consequently faces increased risk of morbidity and mortality. An estimated due date is given by Naegele's rule.
According to the WHO, a preterm birth is defined as "babies born alive before 37 weeks of pregnancy are completed."[22] According to this classification, there are three sub-categories of preterm birth, based on gestational age: extremely preterm (fewer than 28 weeks), very preterm (28 to 32 weeks), moderate to late preterm (32 to 37 weeks).[22] Various jurisdictions may use different classifications.
In classifying perinatal deaths, stillbirths and infant deaths
For most of the 20th century, official definitions of a live birth and infant death in the Soviet Union and Russia differed from common international standards, such as those established by the World Health Organization in the latter part of the century.[23][24] Babies who were fewer than 28 weeks of gestational age, or weighed fewer than 1000grams, or fewer than 35cm in length– even if they showed some sign of life (breathing, heartbeat, voluntary muscle movement)– were classified as "live fetuses" rather than "live births." Only if such newborns survived seven days (168 hours) were they then classified as live births. If, however, they died within that interval, they were classified as stillbirths. If they survived that interval but died within the first 365 days they were classified as infant deaths.
More recently, thresholds for "fetal death" continue to vary widely internationally, sometimes incorporating weight as well as gestational age. The gestational age for statistical recording of fetal deaths ranges from 16 weeks in Norway, to 20 weeks in the US and Australia, 24 weeks in the UK, and 26 weeks in Italy and Spain.[25][26][27]
The WHO defines the perinatal period as "The perinatal period commences at 22 completed weeks (154 days) of gestation and ends seven completed days after birth."[28] Perinatal mortality is the death of fetuses or neonates during the perinatal period. A 2013 study found that "While only a small proportion of births occur before 24 completed weeks of gestation (about 1 per 1000), survival is rare and most of them are either fetal deaths or live births followed by a neonatal death."[25]
Child's gestational age at birth (pregnancy length) is associated with various likely causal maternal non-genetic factors: stress during pregnancy,[30] age, parity, smoking, infection and inflammation, BMI. Also, preexisting maternal medical conditions with genetic component, e.g., diabetes mellitus type1, systemic lupus erythematosus, anaemia. Parental ancestral background (race) also plays a role in pregnancy duration. Gestational age at birth is on average shortened by various pregnancy aspects: twin pregnancy, prelabor rupture of (fetal) membranes, pre-eclampsia, eclampsia, intrauterine growth restriction.[31] The ratio between fetal growth rate and uterine size (reflecting uterine distension) is suspected to partially determine the pregnancy length.[32]
Heritability of pregnancy length
Family-based studies showed that gestational age at birth is partially (25–40%) determined by genetic factors.[33]
↑ Robinson, H. P.; Fleming, J. E. E. (1975). "A Critical Evaluation of Sonar "crown-Rump Length" Measurements". BJOG: An International Journal of Obstetrics and Gynaecology. 82 (9): 702–10. doi:10.1111/j.1471-0528.1975.tb00710.x. PMID1182090. S2CID31663686.
↑ Kędzia, Alicja; Woźniak, Jowita; Ziajkiewicz, Marcin; Dudek, Krzysztof; Derkowski, Wojciech (2009). "Foetal age assessment on the basis of selected parameters of head and trunk". The computer-aided scientific research. Vol.16. Wrocław Scientific Society. pp.241–246. ISBN978-83-7374-060-0.
↑ Snell, BJ (Nov–Dec 2009). "Assessment and management of bleeding in the first trimester of pregnancy". Journal of Midwifery & Women's Health. 54 (6): 483–91. doi:10.1016/j.jmwh.2009.08.007. PMID19879521.
1 2 Hoffman, Caroline S.; Messer, Lynne C.; Mendola, Pauline; Savitz, David A.; Herring, Amy H.; Hartmann, Katherine E. (2008). "Comparison of gestational age at birth based on last menstrual period and ultrasound during the first trimester". Paediatric and Perinatal Epidemiology. 22 (6): 587–596. doi:10.1111/j.1365-3016.2008.00965.x. ISSN0269-5022. PMID19000297.
The American College of Obstetricians and Gynecologists (September 2002). "ACOG Practice Bulletin: Clinical Management Guidelines for Obstetrcian-Gynecologists: Number 38, September 2002. Perinatal care at the threshold of viability". Obstet Gynecol. 100 (3): 617–24. doi:10.1016/S0029-7844(02)02260-3. PMID12220792.
↑ Verlato, Giovanna; Gobber, Daniela; Drago, Donatella; Chiandetti, Lino; Drigo, Paola; Working Group of Intensive Care in the Delivery Room of Extremely Premature Newborns (2016). "Guidelines for Resuscitation in the Delivery Room of Extremely Preterm Infants". Journal of Child Neurology. 19 (1): 31–4. doi:10.1177/088307380401900106011. PMID15032380. S2CID20200767.
↑ Anderson, Barbara A; Silver, Brian D (1986). "Infant Mortality in the Soviet Union: Regional Differences and Measurement Issues". Population and Development Review. 12 (4): 705–38. doi:10.2307/1973432. JSTOR1973432.
↑ Li, Z; Zeki, R; Hilder, L; Sullivan, EA (2012). "Australia's Mothers and Babies 2010". Perinatal statistics series no. 27. Cat. no. PER 57. Australian Institute of Health and Welfare National Perinatal Statistics Unit, Australian Government. Retrieved 4 July 2013.
↑ Clausson, Britt; Lichtenstein, Paul; Cnattingius, Sven (2000). "Genetic influence on birthweight and gestational length determined by studies in offspring of twins". BJOG. 107 (3): 375–81. doi:10.1111/j.1471-0528.2000.tb13234.x. PMID10740335. S2CID43470321.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.
 By gestational sac diameter
By gestational sac diameter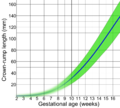 By crown-rump length (CRL)
By crown-rump length (CRL) By biparietal diameter (BPD)
By biparietal diameter (BPD)




