
Far-sightedness, also known as long-sightedness, hypermetropia, and hyperopia, is a condition of the eye where distant objects are seen clearly but near objects appear blurred. This blur is due to incoming light being focused behind, instead of on, the retina due to insufficient accommodation by the lens. Minor hypermetropia in young patients is usually corrected by their accommodation, without any defects in vision. But, due to this accommodative effort for distant vision, people may complain of eye strain during prolonged reading. If the hypermetropia is high, there will be defective vision for both distance and near. People may also experience accommodative dysfunction, binocular dysfunction, amblyopia, and strabismus. Newborns are almost invariably hypermetropic, but it gradually decreases as the newborn gets older.
Orthoptics is a profession allied to the eye care profession. Orthoptists are the experts in diagnosing and treating defects in eye movements and problems with how the eyes work together, called binocular vision. These can be caused by issues with the muscles around the eyes or defects in the nerves enabling the brain to communicate with the eyes. Orthoptists are responsible for the diagnosis and non-surgical management of strabismus (cross-eyed), amblyopia and eye movement disorders. The word orthoptics comes from the Greek words ὀρθός orthos, "straight" and ὀπτικός optikοs, "relating to sight" and much of the practice of orthoptists concerns disorders of binocular vision and defects of eye movement. Orthoptists are trained professionals who specialize in orthoptic treatment, such as eye patches, eye exercises, prisms or glasses. They commonly work with paediatric patients and also adult patients with neurological conditions such as stroke, brain tumours or multiple sclerosis. With specific training, in some countries orthoptists may be involved in monitoring of some forms of eye disease, such as glaucoma, cataract screening and diabetic retinopathy.

Strabismus is a vision disorder in which the eyes do not properly align with each other when looking at an object. The eye that is pointed at an object can alternate. The condition may be present occasionally or constantly. If present during a large part of childhood, it may result in amblyopia, or lazy eyes, and loss of depth perception. If onset is during adulthood, it is more likely to result in double vision.
Anisometropia is a condition in which a person's eyes have substantially differing refractive power. Generally, a difference in power of one diopter (1D) is the threshold for diagnosis of the condition. Patients may have up to 3D of anisometropia before the condition becomes clinically significant due to headache, eye strain, double vision or photophobia.

Diplopia is the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. Also called double vision, it is a loss of visual focus under regular conditions, and is often voluntary. However, when occurring involuntarily, it results from impaired function of the extraocular muscles, where both eyes are still functional, but they cannot turn to target the desired object. Problems with these muscles may be due to mechanical problems, disorders of the neuromuscular junction, disorders of the cranial nerves that innervate the muscles, and occasionally disorders involving the supranuclear oculomotor pathways or ingestion of toxins.
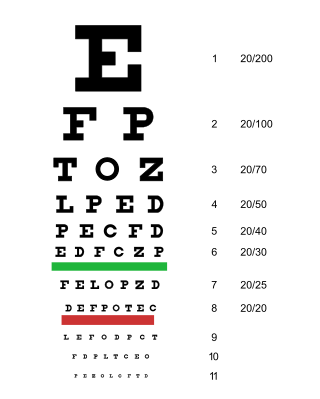
An eye examination is a series of tests performed to assess vision and ability to focus on and discern objects. It also includes other tests and examinations pertaining to the eyes. Eye examinations are primarily performed by an optometrist, ophthalmologist, or an orthoptist. Health care professionals often recommend that all people should have periodic and thorough eye examinations as part of routine primary care, especially since many eye diseases are asymptomatic.
Pediatric ophthalmology is a sub-speciality of ophthalmology concerned with eye diseases, visual development, and vision care in children.
Vision therapy (VT), or behavioral optometry, is an umbrella term for alternative medicine treatments using eye exercises, based around the pseudoscientific claim that vision problems are the true underlying cause of learning difficulties, particularly in children. Vision therapy has not been shown to be effective using scientific studies, except for helping with convergence insufficiency. Most claims—for example that the therapy can address neurological, educational, and spatial difficulties—lack supporting evidence. Neither the American Academy of Pediatrics nor the American Academy of Ophthalmology support the use of vision therapy.

A vergence is the simultaneous movement of both eyes in opposite directions to obtain or maintain single binocular vision.

Exotropia is a form of strabismus where the eyes are deviated outward. It is the opposite of esotropia and usually involves more severe axis deviation than exophoria. People with exotropia often experience crossed diplopia. Intermittent exotropia is a fairly common condition. "Sensory exotropia" occurs in the presence of poor vision in one eye. Infantile exotropia is seen during the first year of life, and is less common than "essential exotropia" which usually becomes apparent several years later.

Sixth nerve palsy, or abducens nerve palsy, is a disorder associated with dysfunction of cranial nerve VI, which is responsible for causing contraction of the lateral rectus muscle to abduct the eye. The inability of an eye to turn outward, results in a convergent strabismus or esotropia of which the primary symptom is diplopia in which the two images appear side-by-side. Thus, the diplopia is horizontal and worse in the distance. Diplopia is also increased on looking to the affected side and is partly caused by overaction of the medial rectus on the unaffected side as it tries to provide the extra innervation to the affected lateral rectus. These two muscles are synergists or "yoke muscles" as both attempt to move the eye over to the left or right. The condition is commonly unilateral but can also occur bilaterally.
Suppression of an eye is a subconscious adaptation by a person's brain to eliminate the symptoms of disorders of binocular vision such as strabismus, convergence insufficiency and aniseikonia. The brain can eliminate double vision by ignoring all or part of the image of one of the eyes. The area of a person's visual field that is suppressed is called the suppression scotoma. Suppression can lead to amblyopia.

Hypertropia is a condition of misalignment of the eyes (strabismus), whereby the visual axis of one eye is higher than the fellow fixating eye. Hypotropia is the similar condition, focus being on the eye with the visual axis lower than the fellow fixating eye. Dissociated vertical deviation is a special type of hypertropia leading to slow upward drift of one or rarely both eyes, usually when the patient is inattentive.

Strabismus surgery is surgery on the extraocular muscles to correct strabismus, the misalignment of the eyes. Strabismus surgery is a one-day procedure that is usually performed under general anesthesia most commonly by either a neuro- or pediatric ophthalmologist. The patient spends only a few hours in the hospital with minimal preoperative preparation. After surgery, the patient should expect soreness and redness but is generally free to return home.

Emmetropia is the state of vision in which a faraway object at infinity is in sharp focus with the ciliary muscle in a relaxed state. That condition of the normal eye is achieved when the refractive power of the cornea and eye lens and the axial length of the eye balance out, which focuses rays exactly on the retina, resulting in perfectly sharp distance vision. A human eye in a state of emmetropia requires no corrective lenses for distance; the vision scores well on a visual acuity test.
Infantile esotropia is an ocular condition of early onset in which one or either eye turns inward. It is a specific sub-type of esotropia and has been a subject of much debate amongst ophthalmologists with regard to its naming, diagnostic features, and treatment.
Dissociated vertical deviation (DVD) is an eye condition which occurs in association with a squint, typically infantile esotropia. The exact cause is unknown, although it is logical to assume it is from faulty innervation of eye muscles.

Stereopsis recovery, also recovery from stereoblindness, is the phenomenon of a stereoblind person gaining partial or full ability of stereo vision (stereopsis).
Botulinum toxin therapy of strabismus is a medical technique used sometimes in the management of strabismus, in which botulinum toxin is injected into selected extraocular muscles in order to reduce the misalignment of the eyes. The injection of the toxin to treat strabismus, reported upon in 1981, is considered to be the first ever use of botulinum toxin for therapeutic purposes. Today, the injection of botulinum toxin into the muscles that surround the eyes is one of the available options in the management of strabismus. Other options for strabismus management are vision therapy and occlusion therapy, corrective glasses and prism glasses, and strabismus surgery.
The management of strabismus may include the use of drugs or surgery to correct the strabismus. Agents used include paralytic agents such as botox used on extraocular muscles, topical autonomic nervous system agents to alter the refractive index in the eyes, and agents that act in the central nervous system to correct amblyopia.


