
An abscess is a collection of pus that has built up within the tissue of the body. Signs and symptoms of abscesses include redness, pain, warmth, and swelling. The swelling may feel fluid-filled when pressed. The area of redness often extends beyond the swelling. Carbuncles and boils are types of abscess that often involve hair follicles, with carbuncles being larger. A cyst is related to an abscess, but it contains a material other than pus, and a cyst has a clearly defined wall.
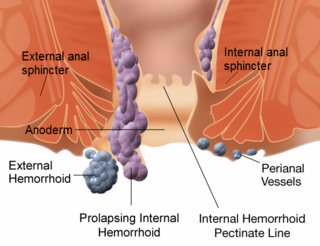
Hemorrhoids, also known as piles, are vascular structures in the anal canal. In their normal state, they are cushions that help with stool control. They become a disease when swollen or inflamed; the unqualified term hemorrhoid is often used to refer to the disease. The signs and symptoms of hemorrhoids depend on the type present. Internal hemorrhoids often result in painless, bright red rectal bleeding when defecating. External hemorrhoids often result in pain and swelling in the area of the anus. If bleeding occurs, it is usually darker. Symptoms frequently get better after a few days. A skin tag may remain after the healing of an external hemorrhoid.

Fecal incontinence (FI), or in some forms, encopresis, is a lack of control over defecation, leading to involuntary loss of bowel contents, both liquid stool elements and mucus, or solid feces. When this loss includes flatus (gas), it is referred to as anal incontinence. FI is a sign or a symptom, not a diagnosis. Incontinence can result from different causes and might occur with either constipation or diarrhea. Continence is maintained by several interrelated factors, including the anal sampling mechanism, and incontinence usually results from a deficiency of multiple mechanisms. The most common causes are thought to be immediate or delayed damage from childbirth, complications from prior anorectal surgery, altered bowel habits. An estimated 2.2% of community-dwelling adults are affected. However, reported prevalence figures vary. A prevalence of 8.39% among non-institutionalized U.S adults between 2005 and 2010 has been reported, and among institutionalized elders figures come close to 50%.
In anatomy, a fistula is an abnormal connection joining two hollow spaces, such as blood vessels, intestines, or other hollow organs to each other, often resulting in an abnormal flow of fluid from one space to the other. An anal fistula connects the anal canal to the perianal skin. An anovaginal or rectovaginal fistula is a hole joining the anus or rectum to the vagina. A colovaginal fistula joins the space in the colon to that in the vagina. A urinary tract fistula is an abnormal opening in the urinary tract or an abnormal connection between the urinary tract and another organ. An abnormal communication between the bladder and the uterus is called a vesicouterine fistula, while if it is between the bladder and the vagina it is known as a vesicovaginal fistula, and if between the urethra and the vagina: a urethrovaginal fistula. When occurring between two parts of the intestine, it is known as an enteroenteral fistula, between the small intestine and the skin as an enterocutaneous fistula, and between the colon and the skin as a colocutaneous fistula.

A rectal prolapse occurs when walls of the rectum have prolapsed to such a degree that they protrude out of the anus and are visible outside the body. However, most researchers agree that there are 3 to 5 different types of rectal prolapse, depending on whether the prolapsed section is visible externally, and whether the full or only partial thickness of the rectal wall is involved.
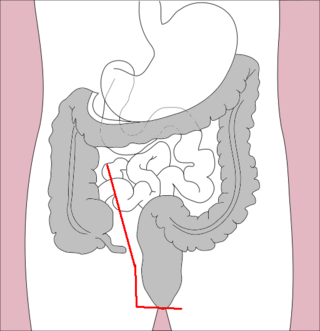
Colorectal surgery is a field in medicine dealing with disorders of the rectum, anus, and colon. The field is also known as proctology, but this term is now used infrequently within medicine and is most often employed to identify practices relating to the anus and rectum in particular. The word proctology is derived from the Greek words πρωκτός proktos, meaning "anus" or "hindparts", and -λογία -logia, meaning "science" or "study".
Proctitis is an inflammation of the anus and the lining of the rectum, affecting only the last 6 inches of the rectum.
Rectal bleeding refers to bleeding in the rectum. There are many causes of rectal hemorrhage, including inflamed hemorrhoids, rectal varices, proctitis, stercoral ulcers and infections. Diagnosis is usually made by proctoscopy, which is an endoscopic test.

Anal fistula is a chronic abnormal communication between the anal canal and the perianal skin. An anal fistula can be described as a narrow tunnel with its internal opening in the anal canal and its external opening in the skin near the anus. Anal fistulae commonly occur in people with a history of anal abscesses. They can form when anal abscesses do not heal properly.

An anoscopy is an examination using a small, rigid, tubular instrument called an anoscope. This is inserted a few inches into the anus in order to evaluate problems of the anal canal. Anoscopy is used to diagnose hemorrhoids, anal fissures, and some cancers.

Stapled hemorrhoidopexy is a surgical procedure that involves the cutting and removal of anal hemorrhoidal vascular cushion, whose function is to help to seal stools and create continence. Procedure also removes abnormally enlarged hemorrhoidal tissue, followed by the repositioning of the remaining hemorrhoidal tissue back to its normal anatomic position. Severe cases of hemorrhoidal prolapse will normally require surgery. Newer surgical procedures include stapled transanal rectal resection (STARR) and procedure for prolapse and hemorrhoids (PPH). Both STARR and PPH are contraindicated in persons with either enterocele or anismus.
Proctocolectomy is the surgical removal of the entire colon and rectum from the human body, leaving the patients small intestine disconnected from their anus. It is a major surgery that is performed by colorectal surgeons, however some portions of the surgery, specifically the colectomy may be performed by general surgeons. It was first performed in 1978 and since that time, medical advancements have led to the surgery being less invasive with great improvements in patient outcomes. The procedure is most commonly indicated for severe forms of inflammatory bowel disease such as ulcerative colitis and Crohn's disease. It is also the treatment of choice for patients with familial adenomatous polyposis.
Perianal hematoma is a hematoma located in, or on the border of the anus. It is sometimes inappropriately referred to as an external hemorrhoid.

In humans, the anus is the external opening of the rectum located inside the intergluteal cleft. Two sphincters control the exit of feces from the body during an act of defecation, which is the primary function of the anus. These are the internal anal sphincter and the external anal sphincter, which are circular muscles that normally maintain constriction of the orifice and which relax as required by normal physiological functioning. The inner sphincter is involuntary and the outer is voluntary. Above the anus is the perineum, which is also located beneath the vulva or scrotum.
Rectal pain is the symptom of pain in the area of the rectum. A number of different causes (68) have been documented.
Rectal discharge is intermittent or continuous expression of liquid from the anus. Normal rectal mucus is needed for proper excretion of waste. Otherwise, this is closely related to types of fecal incontinence but the term rectal discharge does not necessarily imply degrees of incontinence. Types of fecal incontinence that produce a liquid leakage could be thought of as a type of rectal discharge.
Obstructed defecation syndrome is a major cause of functional constipation, of which it is considered a subtype. It is characterized by difficult and/or incomplete emptying of the rectum with or without an actual reduction in the number of bowel movements per week. Normal definitions of functional constipation include infrequent bowel movements and hard stools. In contrast, ODS may occur with frequent bowel movements and even with soft stools, and the colonic transit time may be normal, but delayed in the rectum and sigmoid colon.

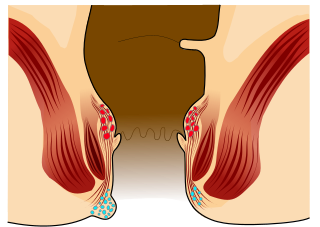
Anorectal disorders include conditions involving the anorectal junction as seen in the image. They are painful but common conditions like hemorrhoids, tears, fistulas, or abscesses that affect the anal region. Most people experience some form of anorectal disorder during their lifetime. Primary care physicians can treat most of these disorders, however, high-risk individuals include those with HIV, roughly half of whom need surgery to remedy the disorders. Likelihood of malignancy should also be considered in high risk individuals. This is why it is important to perform a full history and physical exam on each patient. Because these disorders affect the rectum, people are often embarrassed or afraid to confer with a medical professional.
Fistulectomy is a surgical procedure where a surgeon completely removes a fistula, an abnormal tract that connects two hollow spaces of the body. In comparison to other procedural options of treating fistulae such as fistulotomies, where a fistula is cut open but not completely removed, and seton placement, where a rubber band seton is passed through the tract and left post-operation as a means to allow drainage of the fistula, fistulectomies are considered to be a more radical approach. The total removal of a fistula may damage nearby structures in the process.
In fecal incontinence (FI), surgery may be carried out if conservative measures alone are not sufficient to control symptoms. There are many surgical options described for FI, and they can be considered in 4 general groups.




