Related Research Articles

Oligoclonal bands (OCBs) are bands of immunoglobulins that are seen when a patient's blood serum, or cerebrospinal fluid (CSF) is analyzed. They are used in the diagnosis of various neurological and blood diseases. Oligoclonal bands are present in the CSF of more than 95% of patients with clinically definite multiple sclerosis.

Nephrotic syndrome is a collection of symptoms due to kidney damage. This includes protein in the urine, low blood albumin levels, high blood lipids, and significant swelling. Other symptoms may include weight gain, feeling tired, and foamy urine. Complications may include blood clots, infections, and high blood pressure.

Cerebral edema is excess accumulation of fluid (edema) in the intracellular or extracellular spaces of the brain. This typically causes impaired nerve function, increased pressure within the skull, and can eventually lead to direct compression of brain tissue and blood vessels. Symptoms vary based on the location and extent of edema and generally include headaches, nausea, vomiting, seizures, drowsiness, visual disturbances, dizziness, and in severe cases, death.

Septic shock is a potentially fatal medical condition that occurs when sepsis, which is organ injury or damage in response to infection, leads to dangerously low blood pressure and abnormalities in cellular metabolism. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) defines septic shock as a subset of sepsis in which particularly profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone. Patients with septic shock can be clinically identified by requiring a vasopressor to maintain a mean arterial pressure of 65 mm Hg or greater and having serum lactate level greater than 2 mmol/L (>18 mg/dL) in the absence of hypovolemia. This combination is associated with hospital mortality rates greater than 40%.

The endothelium is a single layer of squamous endothelial cells that line the interior surface of blood vessels and lymphatic vessels. The endothelium forms an interface between circulating blood or lymph in the lumen and the rest of the vessel wall. Endothelial cells form the barrier between vessels and tissue and control the flow of substances and fluid into and out of a tissue.

Macular edema occurs when fluid and protein deposits collect on or under the macula of the eye and causes it to thicken and swell (edema). The swelling may distort a person's central vision, because the macula holds tightly packed cones that provide sharp, clear, central vision to enable a person to see detail, form, and color that is directly in the centre of the field of view.

Primate erythroparvovirus 1, generally referred to as B19 virus(B19V),parvovirus B19 or sometimes erythrovirus B19, is the first known human virus in the family Parvoviridae, genus Erythroparvovirus; it measures only 23–26 nm in diameter. The name is derived from Latin parvum, meaning small, reflecting the fact that B19 ranks among the smallest DNA viruses. B19 virus is most known for causing disease in the pediatric population; however, it can also affect adults. It is the classic cause of the childhood rash called fifth disease or erythema infectiosum, or "slapped cheek syndrome".
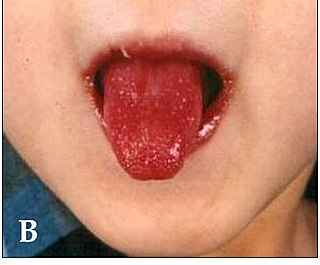
Kawasaki disease is a syndrome of unknown cause that results in a fever and mainly affects children under 5 years of age. It is a form of vasculitis, where medium-sized blood vessels become inflamed throughout the body. The fever typically lasts for more than five days and is not affected by usual medications. Other common symptoms include large lymph nodes in the neck, a rash in the genital area, lips, palms, or soles of the feet, and red eyes. Within three weeks of the onset, the skin from the hands and feet may peel, after which recovery typically occurs. The disease is the leading cause of acquired heart disease in children in developed countries, which include the formation of coronary artery aneurysms and myocarditis.

POEMS syndrome is a rare paraneoplastic syndrome caused by a clone of aberrant plasma cells. The name POEMS is an acronym for some of the disease's major signs and symptoms, as is PEP.

Nephritic syndrome is a syndrome comprising signs of nephritis, which is kidney disease involving inflammation. It often occurs in the glomerulus, where it is called glomerulonephritis. Glomerulonephritis is characterized by inflammation and thinning of the glomerular basement membrane and the occurrence of small pores in the podocytes of the glomerulus. These pores become large enough to permit both proteins and red blood cells to pass into the urine. By contrast, nephrotic syndrome is characterized by proteinuria and a constellation of other symptoms that specifically do not include hematuria. Nephritic syndrome, like nephrotic syndrome, may involve low level of albumin in the blood due to the protein albumin moving from the blood to the urine.
Distributive shock is a medical condition in which abnormal distribution of blood flow in the smallest blood vessels results in inadequate supply of blood to the body's tissues and organs. It is one of four categories of shock, a condition where there is not enough oxygen-carrying blood to meet the metabolic needs of the cells which make up the body's tissues and organs. Distributive shock is different from the other three categories of shock in that it occurs even though the output of the heart is at or above a normal level. The most common cause is sepsis leading to a type of distributive shock called septic shock, a condition that can be fatal.

Hypoalbuminemia is a medical sign in which the level of albumin in the blood is low. This can be due to decreased production in the liver, increased loss in the gastrointestinal tract or kidneys, increased use in the body, or abnormal distribution between body compartments. Patients often present with hypoalbuminemia as a result of another disease process such as malnutrition as a result of severe anorexia nervosa, sepsis, cirrhosis in the liver, nephrotic syndrome in the kidneys, or protein-losing enteropathy in the gastrointestinal tract. One of the roles of albumin is being the major driver of oncotic pressure in the bloodstream and the body. Thus, hypoalbuminemia leads to abnormal distributions of fluids within the body and its compartments. As a result, associated symptoms include edema in the lower legs, ascites in the abdomen, and effusions around internal organs. Laboratory tests aimed at assessing liver function diagnose hypoalbuminemia. Once identified, it is a poor prognostic indicator for patients with a variety of different diseases. Yet, it is only treated in very specific indications in patients with cirrhosis and nephrotic syndrome. Treatment instead focuses on the underlying cause of the hypoalbuminemia. Albumin is an acute negative phase respondent and not a reliable indicator of nutrition status.

Selective immunoglobulin A (IgA) deficiency (SIgAD) is a kind of immunodeficiency, a type of hypogammaglobulinemia. People with this deficiency lack immunoglobulin A (IgA), a type of antibody that protects against infections of the mucous membranes lining the mouth, airways, and digestive tract. It is defined as an undetectable serum IgA level in the presence of normal serum levels of IgG and IgM, in persons older than 4 years. It is the most common of the primary antibody deficiencies. Most such persons remain healthy throughout their lives and are never diagnosed.
Catastrophic antiphospholipid syndrome (CAPS), also known as Asherson's syndrome, is a rare autoimmune disease in which widespread, intravascular clotting causes multi-organ failure. The syndrome is caused by antiphospholipid antibodies that target a group of proteins in the body that are associated with phospholipids. These antibodies activate endothelial cells, platelets, and immune cells, ultimately causing a large inflammatory immune response and widespread clotting. CAPS was first described by Ronald Asherson in 1992. The syndrome exhibits thrombotic microangiopathy, multiple organ thromboses, and in some cases tissue necrosis and is considered an extreme or catastrophic variant of the antiphospholipid syndrome.
Guillain–Barré syndrome (GBS) is a rapid-onset muscle weakness caused by the immune system damaging the peripheral nervous system. Typically, both sides of the body are involved, and the initial symptoms are changes in sensation or pain often in the back along with muscle weakness, beginning in the feet and hands, often spreading to the arms and upper body. The symptoms may develop over hours to a few weeks. During the acute phase, the disorder can be life-threatening, with about 15% of people developing weakness of the breathing muscles and, therefore, requiring mechanical ventilation. Some are affected by changes in the function of the autonomic nervous system, which can lead to dangerous abnormalities in heart rate and blood pressure.
Purple glove syndrome (PGS) is a poorly understood skin disease in which the extremities become swollen, discoloured and painful. PGS is potentially serious and may require amputation. PGS is most common among elderly patients and those receiving multiple large intravenous doses of the epilepsy drug phenytoin. Compartment syndrome is a complication of PGS.

A cerebrospinal fluid leak is a medical condition where the cerebrospinal fluid (CSF) surrounding the brain or spinal cord leaks out of one or more holes or tears in the dura mater. A cerebrospinal fluid leak can be either cranial or spinal, and these are two different disorders. A spinal CSF leak can be caused by one or more meningeal diverticula or CSF-venous fistulas not associated with an epidural leak.
Drug-Induced Aseptic Meningitis (DIAM) is a type of aseptic meningitis related to the use of medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) or biologic drugs such as intravenous immunoglobulin (IVIG). Additionally, this condition generally shows clinical improvement after cessation of the medication, as well as a tendency to relapse with resumption of the medication.

Lupus vasculitis is one of the secondary vasculitides that occurs in approximately 50% of patients with systemic lupus erythematosus (SLE).
Immunoglobulin therapy is the use of a mixture of antibodies to treat several health conditions. These conditions include primary immunodeficiency, immune thrombocytopenic purpura, chronic inflammatory demyelinating polyneuropathy, Kawasaki disease, certain cases of HIV/AIDS and measles, Guillain-Barré syndrome, and certain other infections when a more specific immunoglobulin is not available. Depending on the formulation it can be given by injection into muscle, a vein, or under the skin. The effects last a few weeks.
References
- 1 2 Siddall, Eric; Khatri, Minesh; Radhakrishnan, Jai (16 March 2017). "Capillary leak syndrome: etiologies, pathophysiology, and management". Kidney International. 92 (1): 37–46. doi: 10.1016/j.kint.2016.11.029 . PMID 28318633.
- ↑ Izzedine, Hassan; Mathian, Alexis; Amoura, Zahir; Ng, Jia; Jhaveri, Kenar (25 February 2022). "Anticancer Drug-Induced Capillary Leak Syndrome". Kidney International Reports. 7 (5): 945–953. doi: 10.1016/j.ekir.2022.02.014 . PMC 9091576 . PMID 9091576.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Druey, Kirk M.; Greipp, Philip R. (2010). "Narrative Review: Clarkson Disease-Systemic Capillary Leak Syndrome". Annals of Internal Medicine. 153 (2): 90–8. doi:10.7326/0003-4819-153-2-201007200-00005. PMC 3017349 . PMID 20643990.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Druey, Kirk; Parikh, Samir M. (22 December 2016). "Idiopathic systemic capillary leak syndrome (Clarkson disease)". Journal of Allergy and Clinical Immunology. 140 (3): 663–670. doi:10.1016/j.jaci.2016.10.042. PMC 5481509 . PMID 28012935.
- 1 2 3 4 5 6 7 8 Pineton de Chambrun, Marc; et al. (2017). "The Clinical Picture of Severe Systemic Capillary-Leak Syndrome Episodes Requiring ICU Admission". Critical Care Medicine. 45 (7): 1216–23. doi:10.1097/CCM.0000000000002496. PMID 28622216. S2CID 198448.
- 1 2 3 4 Xie, Zhihui; Gosh, Chandra C.; et al. (2012). "Vascular endothelial hyperpermeability induces the clinical symptoms of Clarkson disease (the systemic capillary leak syndrome)". Blood. 119 (18): 1145–7. doi:10.1182/blood-2011-08-375816. PMC 3359743 . PMID 22411873.
- ↑ Xie, Zhihui; Ghosh, Chandra C.; Parikh, Samir M.; Druey, Kirk M. (2014). "Mechanistic Classification of the Systemic Capillary Leak Syndrome: Clarkson Disease". American Journal of Respiratory and Critical Care Medicine. 189 (9): 1145–7. doi:10.1164/rccm.201310-1746LE. PMC 4098109 . PMID 24787070.
- 1 2 3 Droder, Robert M.; Kyle, Robert A.; Greipp, Philip R. (1992). "Control of systemic capillary leak syndrome with aminophylline and terbutaline". The American Journal of Medicine. 92 (5): 523–6. doi:10.1016/0002-9343(92)90749-2. PMID 1580299.
- ↑ Pecker, Mark; Hammudi, Mustafa; Melchio, Remo; et al. (2 August 2022). "Management of Acute Episodes of Clarkson Disease (Monoclonal Gammopathy-Associated Systemic Capillary Leak Syndrome) With Intravenous Immunoglobulins". AIM Clinical Cases. 1 (6). doi: 10.7326/aimcc.2022.0496 . PMC 9481058 . PMID 36119848.
- ↑ Kapoor, Prashant; Greipp, Patricia T.; Schaefer, Eric W.; Mandrekar, Sumithra J.; Kamal, Arif H.; Gonzalez-Paz, Natalia C.; Kumar, Shaji; Greipp, Philip R. (2010). "Idiopathic Systemic Capillary Leak Syndrome (Clarkson's Disease): The Mayo Clinic Experience". Mayo Clinic Proceedings. 85 (10): 905–12. doi:10.4065/mcp.2010.0159. PMC 2947962 . PMID 20634497.
- 1 2 3 4 Xie, Zhihui; Chan, Eunice; et al. (2015). "High dose intravenous immunoglobulin therapy of the Systemic Capillary Leak Syndrome (Clarkson disease)". The American Journal of Medicine. 128 (1): 91–5. doi:10.1016/j.amjmed.2014.08.015. PMC 4282822 . PMID 25193271.
- 1 2 3 4 5 6 Pineton de Chambrun, Marc; et al. (June 8, 2017). "Intravenous immunoglobulins improve survival in monoclonal gammopathy-associated systemic capillary-leak syndrome". The American Journal of Medicine. 130 (10): 1219.e19–1219.e27. doi: 10.1016/j.amjmed.2017.05.023 . PMID 28602874.
- 1 2 Lambert, Marc; Launay, David; Hachulla, Eric; Morell-Dubois, Sandrine; Soland, Vincent; Queyrel, Viviane; Fourrier, François; Hatron, Pierre-Yves (2008). "High-dose intravenous immunoglobulins dramatically reverse systemic capillary leak syndrome". Critical Care Medicine. 36 (7): 2184–7. doi:10.1097/CCM.0b013e31817d7c71. PMID 18552679. S2CID 41357732.
- ↑ Moyon, Quentin; et al. (2022). "Intravenous Immunoglobulins Tapering and Withdrawal in Systemic Capillary Leak Syndrome (Clarkson Disease)". The Journal of Allergy and Clinical Immunology:In Practice. 10 (11): 2889–95. doi: 10.1016/j.jaip.2022.07.006 . PMID 35870726. S2CID 250970743.
- ↑ Clarkson, Bayard; Thompson, David; Horwith, Melvin; Luckey, E.Hugh (1960). "Cyclical edema and shock due to increased capillary permeability". The American Journal of Medicine. 29 (2): 193–216. doi:10.1016/0002-9343(60)90018-8. PMID 13693909.