Related Research Articles

In aphasia, a person may be unable to comprehend or unable to formulate language because of damage to specific brain regions. The major causes are stroke and head trauma; prevalence is hard to determine but aphasia due to stroke is estimated to be 0.1–0.4% in the Global North. Aphasia can also be the result of brain tumors, epilepsy, autoimmune neurological diseases, brain infections, or neurodegenerative diseases.

Expressive aphasia, also known as Broca's aphasia, is a type of aphasia characterized by partial loss of the ability to produce language, although comprehension generally remains intact. A person with expressive aphasia will exhibit effortful speech. Speech generally includes important content words but leaves out function words that have more grammatical significance than physical meaning, such as prepositions and articles. This is known as "telegraphic speech". The person's intended message may still be understood, but their sentence will not be grammatically correct. In very severe forms of expressive aphasia, a person may only speak using single word utterances. Typically, comprehension is mildly to moderately impaired in expressive aphasia due to difficulty understanding complex grammar.

In neuroscience and psychology, the term language center refers collectively to the areas of the brain which serve a particular function for speech processing and production. Language is a core system that gives humans the capacity to solve difficult problems and provides them with a unique type of social interaction. Language allows individuals to attribute symbols to specific concepts, and utilize them through sentences and phrases that follow proper grammatical rules. Finally, speech is the mechanism by which language is orally expressed.
Wernicke's aphasia, also known as receptive aphasia, sensory aphasia, fluent aphasia, or posterior aphasia, is a type of aphasia in which individuals have difficulty understanding written and spoken language. Patients with Wernicke's aphasia demonstrate fluent speech, which is characterized by typical speech rate, intact syntactic abilities and effortless speech output. Writing often reflects speech in that it tends to lack content or meaning. In most cases, motor deficits do not occur in individuals with Wernicke's aphasia. Therefore, they may produce a large amount of speech without much meaning. Individuals with Wernicke's aphasia are typically unaware of their errors in speech and do not realize their speech may lack meaning. They typically remain unaware of even their most profound language deficits.

Broca's area, or the Broca area, is a region in the frontal lobe of the dominant hemisphere, usually the left, of the brain with functions linked to speech production.
Aphasiology is the study of language impairment usually resulting from brain damage, due to neurovascular accident—hemorrhage, stroke—or associated with a variety of neurodegenerative diseases, including different types of dementia. These specific language deficits, termed aphasias, may be defined as impairments of language production or comprehension that cannot be attributed to trivial causes such as deafness or oral paralysis. A number of aphasias have been described, but two are best known: expressive aphasia and receptive aphasia.

Neuropsychology is a branch of psychology concerned with how a person's cognition and behavior are related to the brain and the rest of the nervous system. Professionals in this branch of psychology focus on how injuries or illnesses of the brain affect cognitive and behavioral functions.
Anomic aphasia is a mild, fluent type of aphasia where individuals have word retrieval failures and cannot express the words they want to say. By contrast, anomia is a deficit of expressive language, and a symptom of all forms of aphasia, but patients whose primary deficit is word retrieval are diagnosed with anomic aphasia. Individuals with aphasia who display anomia can often describe an object in detail and maybe even use hand gestures to demonstrate how the object is used, but cannot find the appropriate word to name the object. Patients with anomic aphasia have relatively preserved speech fluency, repetition, comprehension, and grammatical speech.
Cognitive neuropsychology is a branch of cognitive psychology that aims to understand how the structure and function of the brain relates to specific psychological processes. Cognitive psychology is the science that looks at how mental processes are responsible for the cognitive abilities to store and produce new memories, produce language, recognize people and objects, as well as our ability to reason and problem solve. Cognitive neuropsychology places a particular emphasis on studying the cognitive effects of brain injury or neurological illness with a view to inferring models of normal cognitive functioning. Evidence is based on case studies of individual brain damaged patients who show deficits in brain areas and from patients who exhibit double dissociations. Double dissociations involve two patients and two tasks. One patient is impaired at one task but normal on the other, while the other patient is normal on the first task and impaired on the other. For example, patient A would be poor at reading printed words while still being normal at understanding spoken words, while the patient B would be normal at understanding written words and be poor at understanding spoken words. Scientists can interpret this information to explain how there is a single cognitive module for word comprehension. From studies like these, researchers infer that different areas of the brain are highly specialised. Cognitive neuropsychology can be distinguished from cognitive neuroscience, which is also interested in brain-damaged patients, but is particularly focused on uncovering the neural mechanisms underlying cognitive processes.
Wernicke's area, also called Wernicke's speech area, is one of the two parts of the cerebral cortex that are linked to speech, the other being Broca's area. It is involved in the comprehension of written and spoken language, in contrast to Broca's area, which is primarily involved in the production of language. It is traditionally thought to reside in Brodmann area 22, which is located in the superior temporal gyrus in the dominant cerebral hemisphere, which is the left hemisphere in about 95% of right-handed individuals and 70% of left-handed individuals.
Conduction aphasia, also called associative aphasia, is an uncommon form of difficulty in speaking (aphasia). It is caused by damage to the parietal lobe of the brain. An acquired language disorder, it is characterised by intact auditory comprehension, coherent speech production, but poor speech repetition. Affected people are fully capable of understanding what they are hearing, but fail to encode phonological information for production. This deficit is load-sensitive as the person shows significant difficulty repeating phrases, particularly as the phrases increase in length and complexity and as they stumble over words they are attempting to pronounce. People have frequent errors during spontaneous speech, such as substituting or transposing sounds. They are also aware of their errors and will show significant difficulty correcting them.
CarlWernicke was a German physician, anatomist, psychiatrist and neuropathologist. He is known for his influential research into the pathological effects of specific forms of encephalopathy and also the study of receptive aphasia, both of which are commonly associated with Wernicke's name and referred to as Wernicke encephalopathy and Wernicke's aphasia, respectively. His research, along with that of Paul Broca, led to groundbreaking realizations of the localization of brain function, specifically in speech. As such, Wernicke's area has been named after the scientist.

Global aphasia is a severe form of nonfluent aphasia, caused by damage to the left side of the brain, that affects receptive and expressive language skills as well as auditory and visual comprehension. Acquired impairments of communicative abilities are present across all language modalities, impacting language production, comprehension, and repetition. Patients with global aphasia may be able to verbalize a few short utterances and use non-word neologisms, but their overall production ability is limited. Their ability to repeat words, utterances, or phrases is also affected. Due to the preservation of the right hemisphere, an individual with global aphasia may still be able to express themselves through facial expressions, gestures, and intonation. This type of aphasia often results from a large lesion of the left perisylvian cortex. The lesion is caused by an occlusion of the left middle cerebral artery and is associated with damage to Broca's area, Wernicke's area, and insular regions which are associated with aspects of language.
Transcortical sensory aphasia (TSA) is a kind of aphasia that involves damage to specific areas of the temporal lobe of the brain, resulting in symptoms such as poor auditory comprehension, relatively intact repetition, and fluent speech with semantic paraphasias present. TSA is a fluent aphasia similar to Wernicke's aphasia, with the exception of a strong ability to repeat words and phrases. The person may repeat questions rather than answer them ("echolalia").

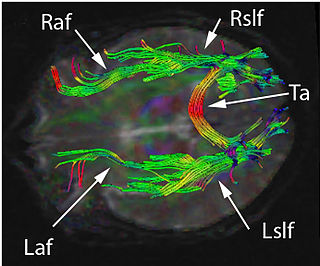
Brodmann area 22 is a Brodmann's area that is cytoarchitecturally located in the posterior superior temporal gyrus of the brain. In the left cerebral hemisphere, it is one portion of Wernicke's area. The left hemisphere BA22 helps with generation and understanding of individual words. On the right side of the brain, BA22 helps to discriminate pitch and sound intensity, both of which are necessary to perceive melody and prosody. Wernicke's area is active in processing language and consists of the left Brodmann area 22 and Brodmann area 40, the supramarginal gyrus.
Transcortical motor aphasia (TMoA), also known as commissural dysphasia or white matter dysphasia, results from damage in the anterior superior frontal lobe of the language-dominant hemisphere. This damage is typically due to cerebrovascular accident (CVA). TMoA is generally characterized by reduced speech output, which is a result of dysfunction of the affected region of the brain. The left hemisphere is usually responsible for performing language functions, although left-handed individuals have been shown to perform language functions using either their left or right hemisphere depending on the individual. The anterior frontal lobes of the language-dominant hemisphere are essential for initiating and maintaining speech. Because of this, individuals with TMoA often present with difficulty in speech maintenance and initiation.

Foix–Chavany–Marie syndrome (FCMS), also known as bilateral opercular syndrome, is a neuropathological disorder characterized by paralysis of the facial, tongue, pharynx, and masticatory muscles of the mouth that aid in chewing. The disorder is primarily caused by thrombotic and embolic strokes, which cause a deficiency of oxygen in the brain. As a result, bilateral lesions may form in the junctions between the frontal lobe and temporal lobe, the parietal lobe and cortical lobe, or the subcortical region of the brain. FCMS may also arise from defects existing at birth that may be inherited or nonhereditary. Symptoms of FCMS can be present in a person of any age and it is diagnosed using automatic-voluntary dissociation assessment, psycholinguistic testing, neuropsychological testing, and brain scanning. Treatment for FCMS depends on the onset, as well as on the severity of symptoms, and it involves a multidisciplinary approach.
The Boston Diagnostic Aphasia Examination is a neuropsychological battery used to evaluate adults suspected of having aphasia, and is currently in its third edition. It was created by Harold Goodglass and Edith Kaplan. The exam evaluates language skills based on perceptual modalities, processing functions, and response modalities. Administration time ranges from 20 to 45 minutes for the shortened version but it can last up to 120 minutes for the extended version of the assessment. There are five subtests which include: conversational & expository speech, auditory comprehension, oral expression, reading, and writing. In the extended version all questions are asked while in the shortened version only a few questions are asked within each subtest. Many other tests are sometimes used by neurologists and speech language pathologists on a case-by-case basis, and other comprehensive tests exist like the Western Aphasia Battery.

Sign language refers to any natural language which uses visual gestures produced by the hands and body language to express meaning. The brain's left side is the dominant side utilized for producing and understanding sign language, just as it is for speech. In 1861, Paul Broca studied patients with the ability to understand spoken languages but the inability to produce them. The damaged area was named Broca's area, and located in the left hemisphere’s inferior frontal gyrus. Soon after, in 1874, Carl Wernicke studied patients with the reverse deficits: patients could produce spoken language, but could not comprehend it. The damaged area was named Wernicke's area, and is located in the left hemisphere’s posterior superior temporal gyrus.
The Boston Process Approach is a neurological assessment tool developed by Edith Kaplan and her colleagues, Harold Goodglass, Nelson Butters, Laird Cermak, and Norman Geschwind at the Boston Veterans Medical Center. The main purpose of the Boston Process Approach is to assess brain damage as well as cognitive impairments in patients through a series of tests that are related to memory, attention, intelligence, and other aspects of information processing. This approach is one of the more flexible and qualitative neurological assessments because it emphasizes how a patient performs a task instead of whether they succeeded or failed at it.
References
- ↑ Kaplan; Goodglass, Harold; Weintraub, Sandra (1983). Boston Naming Test. Philadelphia: Lea & Febiger. OCLC 10450471.
- 1 2 del Toro, Christina M.; Bislick, Lauren P.; Comer, Matthew; Velozo, Craig; Romero, Sergio; Gonzalez Rothi, Leslie J.; Kendall, Diane L. (2010). "Development of a Short Form of the Boston Naming Test for Individuals with Aphasia". Journal of Speech, Language, and Hearing Research. 54 (4): 1089–100. doi:10.1044/1092-4388(2010/09-0119). PMID 21173387.
- 1 2 Nicholas, Linda E.; Brookshire, Robert H.; MacLennan, Donald L.; Schumacher, James G.; Porrazzo, Shirley A. (1988). "The Boston Naming Test: Revised Administration and Scoring Procedures and Normative Information for Non-Brain-Damaged Adults". Clinical Aphasiology. Boston: College-Hill Press. pp. 103–15. ISBN 0-316-71779-7. Archived from the original on Aug 8, 2023 – via The Aphasiology Archive.
- ↑ Goodglass H, Kaplan E, Barresi B: Boston Diagnostic Aphasia Examination, 3rd edition. Austin, TX, Pro-Ed Inc., 2001
- 1 2 Mitchell, Rachel L. C.; Crow, Tim J. (2005). "Right hemisphere language functions and schizophrenia: The forgotten hemisphere?". Brain. 128 (5): 963–78. doi: 10.1093/brain/awh466 . PMID 15743870.
- ↑ Obler, Loraine K.; Rykhlevskaia, Elena; Schnyer, David; Clark-Cotton, Manuella R.; Spiro Iii, Avron; Hyun, Jungmoon; Kim, Dae-Shik; Goral, Mira; Albert, Martin L. (2010). "Bilateral brain regions associated with naming in older adults". Brain and Language. 113 (3): 113–23. doi:10.1016/j.bandl.2010.03.001. PMC 2975055 . PMID 20399492.