Related Research Articles
Granuloma faciale is an uncommon benign chronic skin disease of unknown origin characterized by single or multiple cutaneous nodules, usually occurring over the face. Occasionally, extrafacial involvement is noted, most often on sun-exposed areas.

Pityriasis rubra pilaris refers to a group of chronic disorders characterized by reddish orange, scaling plaques and keratotic follicular papules. Symptoms may include reddish-orange patches on the skin, severe flaking, uncomfortable itching, thickening of the skin on the feet and hands, and thickened bumps around hair follicles. For some, early symptoms may also include generalized swelling of the legs, feet and other parts of the body. PRP has a varied clinical progression and a varied rate of improvement. There is currently no known cause or cure for PRP.

Erythroderma is an inflammatory skin disease with redness and scaling that affects nearly the entire cutaneous surface. This term applies when 90% or more of the skin is affected.

Perioral dermatitis, also known as periorificial dermatitis, is a common type of skin rash. Symptoms include multiple small (1–2 mm) bumps and blisters sometimes with background redness and scale, localized to the skin around the mouth and nostrils. Less commonly the eyes and genitalia may be involved. It can be persistent or recurring and resembles particularly rosacea and to some extent acne and allergic dermatitis. The term "dermatitis" is a misnomer because this is not an eczematous process.

Glochids or glochidia are hair-like spines or short prickles, generally barbed, found on the areoles of cacti in the sub-family Opuntioideae. Cactus glochids easily detach from the plant and lodge in the skin, causing irritation upon contact. The tufts of glochids in the areoles nearly cover the stem surfaces of some cactus species, each tuft containing hundreds of glochids; this may be in addition to, or instead of, the larger, more conspicuous cactus spines, which do not readily detach and are not generally barbed.

Eczema herpeticum is a rare but severe disseminated infection that generally occurs at sites of skin damage produced by, for example, atopic dermatitis, burns, long-term usage of topical steroids or eczema. It is also known as Kaposi varicelliform eruption, Pustulosis varioliformis acute and Kaposi-Juliusberg dermatitis.

Erythema annulare centrifugum (EAC), is a descriptive term for a class of skin lesion presenting redness (erythema) in a ring form (anulare) that spreads from a center (centrifugum). It was first described by Darier in 1916. Many different terms have been used to classify these types of lesions and it is still controversial on what exactly defines EAC. Some of the types include annular erythema, erythema perstans, erythema gyratum perstans, erythema gyratum repens, darier erythema and erythema figuratum perstans.

Pemphigoid is a group of rare autoimmune blistering diseases of the skin, and mucous membranes. As its name indicates, pemphigoid is similar in general appearance to pemphigus, but, unlike pemphigus, pemphigoid does not feature acantholysis, a loss of connections between skin cells.
Acneiform eruptions are a group of dermatoses including acne vulgaris, rosacea, folliculitis, and perioral dermatitis. Restated, acneiform eruptions are follicular eruptions characterized by papules and pustules resembling acne. The hybrid term acneiform, literally, refers to an appearance similar to acne.
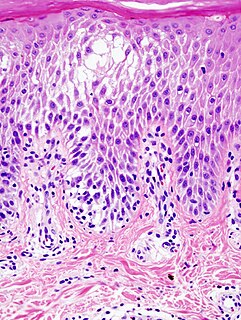
Spongiosis is mainly intercellular edema in the epidermis, and is characteristic of eczematous dermatitis, manifested clinically by intraepidermal vesicles, "juicy" papules, and/or lichenification. It is a severe case of eczema that affects the epidermis, dermis and/or subcutaneous skin tissues. The three types of spongiotic dermatitis are acute, subacute and chronic. A dermatologist can diagnose acute spongiotic dermatitis by examining the skin during an office visit but a biopsy is needed for an accurate diagnosis of the type.
Acne conglobata is a highly inflammatory disease presenting with comedones, nodules, abscesses, and draining sinus tracts.

Neonatal acne, also known as acne neonatorum, is an acneiform eruption that occurs in newborns or infants within the first 4-6 weeks of life, and presents with open and closed comedones on the cheeks, chin and forehead.

Lupus miliaris disseminatus faciei , also known as acne agminata, is a disease with a similar appearance to acne vulgaris. The cause of LMDF is unknown.
Persistent edema of rosacea is a hard, nonpitting edema found on the areas involved, those mainly being the forehead, glabella, upper eyelids, nose, and/or cheeks.
Id reactions are types of acute dermatitis developing after days or weeks at skin locations distant from the initial inflammatory or infectious site. They can be localised or generalised. This is also known as an 'autoeczematous response' and there must be an identifiable initial inflammatory or infectious skin problem which leads to the generalised eczema. Often intensely itchy, the red papules and pustules can also be associated with blisters and scales and are always remote from the primary lesion. It is most commonly a blistering rash with itchy vesicles on the sides of fingers and feet as a reaction to fungal infection on the feet, athlete's foot. Stasis dermatitis, allergic contact dermatitis, acute irritant contact eczema and infective dermatitis have been documented as possible triggers, but the exact cause and mechanism is not fully understood. Several other types of id reactions exist including erythema nodosum, erythema multiforme, Sweet's syndrome and urticaria.

Zirconium granulomas are a skin condition characterized by a papular eruption involving the axillae, and are sometimes considered an allergic reaction to deodorant containing zirconium lactate. They are the result of a delayed granulomatous hypersensitivity reaction, and can also occur from exposure to aluminum zirconium complexes. Commonly, zirconium containing products are used to relieve toxicodendron irritation. The lesions are similar to those from sarcoidosis, and commonly manifest four to six weeks after contact. They appear as erythematous, firm, raised, shiny papules. Corticosteroids are used to ease the inflammation, but curative treatment is currently unavailable.
Benign cephalic histiocytosis not to be confused with "Neonatal cephalic pustulosis" is a rare skin condition affecting boys and girls equally, characterized by skin lesions that initially present on the head in all cases, often the cheeks, eyelids, forehead, and ears.
Infantile acne is a form of acneiform eruption that occurs in infants from 6 weeks to 1 year of age. Typical symptoms include inflammatory and noninflammatory lesions, papules and pustules most commonly present on the face. No cause of infantile acne has been established but it may be caused by increased sebaceous gland secretions due to elevated androgens, genetics and the fetal adrenal gland causing increased sebum production. Infantile acne can resolve by itself by age 1 or 2 however treatment options include topical benzyl peroxide, topical retinoids and topical antibiotics in most cases.

Lip licker's dermatitis, also called irritant contact cheilitis, is a type of skin inflammation around the lips due to saliva from repetitive lip licking. The resulting scaling, redness, chapping and crusting make a well-defined ring around the lips. The rash may extend as far as the tongue can reach and frequently spares the angle of the mouth.
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Dessinioti, C; Antoniou, C; Katsambas, A (January–February 2014). "Acneiform eruptions". Clinics in Dermatology (Review). 32 (1): 24–34. doi:10.1016/j.clindermatol.2013.05.023. PMID 24314375.
- 1 2 3 4 5 6 7 8 9 10 Zalaudek, I; Di Stefani, A; Ferrara, G; Argenziano, G (April 2005). "Childhood granulomatous periorificial dermatitis: a controversial disease". Journal of the German Society of Dermatology (Review). 3 (4): 252–5. doi:10.1111/j.1610-0387.2005.05009.x. PMID 16370472. S2CID 9802651.
- 1 2 3 4 5 6 7 8 9 Kim, YJ; Shin, JW; Lee, JS; Park, YL; Whang, KU; Lee, SY (August 2011). "Childhood granulomatous periorificial dermatitis". Annals of Dermatology (Review). 23 (3): 386–8. doi:10.5021/ad.2011.23.3.386. PMC 3162274 . PMID 21909215.