Related Research Articles

A repetitive strain injury (RSI) is an injury to part of the musculoskeletal or nervous system caused by repetitive use, vibrations, compression or long periods in a fixed position. Other common names include repetitive stress injury, repetitive stress disorders, cumulative trauma disorders (CTDs), and overuse syndrome.

Carpal tunnel syndrome (CTS) is a nerve compression syndrome associated with the collected signs and symptoms of compression of the median nerve at the carpal tunnel in the wrist. Carpal tunnel syndrome is an idiopathic syndrome but there are environmental, and medical risk factors associated with the condition. CTS can affect both wrists.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.
Pudendal nerve entrapment (PNE), also known as Alcock canal syndrome, is an uncommon source of chronic pain in which the pudendal nerve is entrapped or compressed in Alcock's canal. There are several different types of PNE based on the site of entrapment anatomically. Pain is positional and is worsened by sitting. Other symptoms include genital numbness, fecal incontinence and urinary incontinence.

Phalen's maneuver is a diagnostic test for carpal tunnel syndrome by an American orthopedist named George S. Phalen.

Tinel's sign is a way to detect irritated nerves. It is performed by lightly tapping (percussing) over the nerve to elicit a sensation of tingling or "pins and needles" in the distribution of the nerve. Percussion is usually performed moving distal to proximal. It is named after Jules Tinel.

Tarsal tunnel syndrome (TTS) is a nerve compression syndrome or nerve entrapment syndrome causing a painful foot condition in which the tibial nerve is entrapped as it travels through the tarsal tunnel. The tarsal tunnel is found along the inner leg behind the medial malleolus. The posterior tibial artery, tibial nerve, and tendons of the tibialis posterior, flexor digitorum longus, and flexor hallucis longus muscles travel in a bundle through the tarsal tunnel. Inside the tunnel, the nerve splits into three segments. One nerve (calcaneal) continues to the heel, the other two continue on to the bottom of the foot. The tarsal tunnel is delineated by bone on the inside and the flexor retinaculum on the outside.

The flexor retinaculum is a fibrous band on the palmar side of the hand near the wrist. It arches over the carpal bones of the hands, covering them and forming the carpal tunnel.

The recurrent branch of the median nerve is the branch of the median nerve which supplies the thenar muscles. It is also occasionally referred to as the thenar branch of the median nerve, or the thenar muscular branch of the median nerve.

In the human body, the carpal tunnel or carpal canal is a flattened body cavity on the flexor (palmar/volar) side of the wrist, bounded by the carpal bones and flexor retinaculum. It forms the passageway that transmits the median nerve and the tendons of the extrinsic flexor muscles of the hand from the forearm to the hand. The median artery is an anatomical variant. When present it lies between the radial artery, and the ulnar artery and runs with the median nerve supplying the same structures innervated.

Idiopathic ulnar neuropathy at the elbow is a condition where pressure on the ulnar nerve as it passes through the cubital tunnel causes ulnar neuropathy. The symptoms of neuropathy are paresthesia (tingling) and numbness primarily affecting the little finger and ring finger of the hand. Ulnar neuropathy can progress to weakness and atrophy of the muscles in the hand. Symptoms can be alleviated by the use of a splint to prevent the elbow from flexing while sleeping.

Radial tunnel syndrome (RTS) is a compression neuropathy of the radial nerve as it travels from the upper arm to the hand and wrist.
Ulnar neuropathy is a disorder involving the ulnar nerve. Ulnar neuropathy may be caused by entrapment of the ulnar nerve with resultant numbness and tingling. It may also cause weakness or paralysis of the muscles supplied by the nerve. Ulnar neuropathy may affect the elbow as cubital tunnel syndrome. At the wrist a similar neuropathy is ulnar tunnel syndrome.
Neural fibrolipoma is an overgrowth of fibro-fatty tissue along a nerve trunk that often leads to nerve compression. These only occur in the extremities, and often affect the median nerve. They are rare, very slow-growing, and their origin is unknown. It is believed that they may begin growth in response to trauma. They are not encapsulated by any sort of covering or sheath around the growth itself, as opposed to other cysts beneath the skin that often are. This means there are loosely defined margins of this lipoma. Despite this, they are known to be benign. Neural fibrolipomas are often more firm and tough to the touch than other lipomas. They are slightly mobile under the skin, and compress with pressure.

Nerve compression syndrome, or compression neuropathy, or nerve entrapment syndrome, is a medical condition caused by chronic, direct pressure on a peripheral nerve. It is known colloquially as a trapped nerve, though this may also refer to nerve root compression. Its symptoms include pain, tingling, numbness and muscle weakness. The symptoms affect just one particular part of the body, depending on which nerve is affected. The diagnosis is largely clinical and can be confirmed with diagnostic nerve blocks. Occasionally imaging and electrophysiology studies aid in the diagnosis. Timely diagnosis is important as untreated chronic nerve compression may cause permanent damage. A surgical nerve decompression can relieve pressure on the nerve but cannot always reverse the physiological changes that occurred before treatment. Nerve injury by a single episode of physical trauma is in one sense an acute compression neuropathy but is not usually included under this heading, as chronic compression takes a unique pathophysiological course.
Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.
This article is about physical therapy in carpal tunnel syndrome.

Carpal tunnel surgery, also called carpal tunnel release (CTR) and carpal tunnel decompression surgery, is a nerve decompression in which the transverse carpal ligament is divided. It is a surgical treatment for carpal tunnel syndrome (CTS) and recommended when there is constant (not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting no longer controls intermittent symptoms of pain in the carpal tunnel. In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment. Approximately 500,000 surgical procedures are performed each year, and the economic impact of this condition is estimated to exceed $2 billion annually.
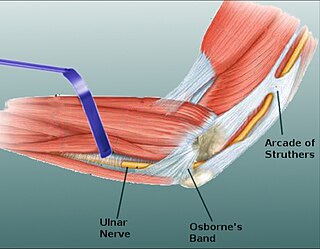
Osborne's ligament, also Osborne's band, Osborne's fascia, Osborne's arcade, arcuate ligament of Osborne, or the cubital tunnel retinaculum, refers to either the connective tissue which spans the humeral and ulnar heads of the flexor carpi ulnaris (FCU) or another distinct tissue located between the olecranon process of the ulna and the medial epicondyle of the humerus. It is named after Geoffrey Vaughan Osborne, a British orthopedic surgeon, who described the eponymous tissue in 1957.
A nerve decompression is a neurosurgical procedure to relieve chronic, direct pressure on a nerve to treat nerve entrapment, a pain syndrome characterized by severe chronic pain and muscle weakness. In this way a nerve decompression targets the underlying pathophysiology of the syndrome and is considered a first-line surgical treatment option for peripheral nerve pain. Despite treating the underlying cause of the disease, the symptoms may not be fully reversible as delays in diagnosis can allow permanent damage to occur to the nerve and surrounding microvasculature. Traditionally only nerves accessible with open surgery have been good candidates, however innovations in laparoscopy and nerve-sparing techniques made nearly all nerves in the body good candidates, as surgical access is no longer a barrier.
References
- 1 2 Robert R. Slater, Jr; . M.D. (1999), Carpal Tunnel Syndrome: Current Concepts , retrieved 2010-05-04
- 1 2 Carpal Compression Test, 2008, retrieved 2010-05-04
- ↑ González Del Pino, J.; Delgado-Martínez, A. D.; González González, I.; Lovic, A. (1997), "Value of the Carpal Compression Test in the Diagnosis of Carpal Tunnel Syndrome", Journal of Hand Surgery (British and European Volume), 22 (1): 38–41, doi:10.1016/s0266-7681(97)80012-5, PMID 9061521, S2CID 25924364 , retrieved 2010-05-04
- ↑ Durkan, J.A. (1991), "A new diagnostic test for carpal tunnel syndrome", The Journal of Bone and Joint Surgery, 73 (4): 535–538, doi:10.2106/00004623-199173040-00009, PMID 1796937, archived from the original on 2010-03-05, retrieved 2010-05-04