
The human leg, in the general word sense, is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or gluteal region. However, the definition in human anatomy refers only to the section of the lower limb extending from the knee to the ankle, also known as the crus or, especially in non-technical use, the shank. Legs are used for standing, and all forms of locomotion including recreational such as dancing, and constitute a significant portion of a person's mass. Female legs generally have greater hip anteversion and tibiofemoral angles, but shorter femur and tibial lengths than those in males.

A gait is a pattern of limb movements made during locomotion. Human gaits are the various ways in which a human can move, either naturally or as a result of specialized training. Human gait is defined as bipedal, biphasic forward propulsion of the center of gravity of the human body, in which there are alternate sinuous movements of different segments of the body with least expenditure of energy. Different gait patterns are characterized by differences in limb-movement patterns, overall velocity, forces, kinetic and potential energy cycles, and changes in the contact with the ground.

Lordosis is historically defined as an abnormal inward curvature of the lumbar spine. However, the terms lordosis and lordotic are also used to refer to the normal inward curvature of the lumbar and cervical regions of the human spine. Similarly, kyphosis historically refers to abnormal convex curvature of the spine. The normal outward (convex) curvature in the thoracic and sacral regions is also termed kyphosis or kyphotic. The term comes from the Greek lordōsis, from lordos.

Spondylolisthesis is the displacement of one spinal vertebra compared to another. While some medical dictionaries define spondylolisthesis specifically as the forward or anterior displacement of a vertebra over the vertebra inferior to it, it is often defined in medical textbooks as displacement in any direction. Spondylolisthesis is graded based upon the degree of slippage of one vertebral body relative to the subsequent adjacent vertebral body. Spondylolisthesis is classified as one of the six major etiologies: degenerative, traumatic, dysplastic, isthmic, pathologic, or post-surgical. Spondylolisthesis most commonly occurs in the lumbar spine, primarily at the L5-S1 level with the L5 vertebral body anteriorly translating over the S1 vertebral body.

Trendelenburg's sign is found in people with weak or paralyzed abductor muscles of the hip, namely gluteus medius and gluteus minimus. It is named after the German surgeon Friedrich Trendelenburg. It is often incorrectly referenced as the Trendelenburg test which is a test for vascular insufficiency in the lower extremities.
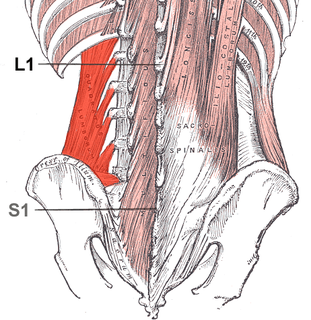
The quadratus lumborum muscle, informally called the QL, is a paired muscle of the left and right posterior abdominal wall. It is the deepest abdominal muscle, and commonly referred to as a back muscle. Each is irregular and quadrilateral in shape.

Trendelenburg gait, named after Friedrich Trendelenburg, is an abnormal gait. It is caused by weakness or ineffective action of the gluteus medius muscle and the gluteus minimus muscle.
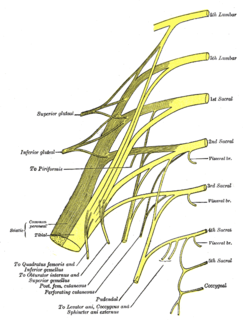
The inferior gluteal nerve is the main motor neuron that innervates the gluteus maximus muscle. It is responsible for the movement of the gluteus maximus in activities requiring the hip to extend the thigh, such as climbing stairs. Injury to this nerve is rare but often occurs as a complication of posterior approach to the hip during hip replacement. When damaged, one would develop gluteus maximus lurch, which is a gait abnormality which causes the individual to 'lurch' backwards to compensate lack in hip extension.
The knee examination, in medicine and physiotherapy, is performed as part of a physical examination, or when a patient presents with knee pain or a history that suggests a pathology of the knee joint.

The acetabular labrum is a ring of cartilage that surrounds the acetabulum of the hip. The anterior portion is most vulnerable when the labrum tears.

Pubic symphysis diastasis is the separation of normally joined pubic bones, as in the dislocation of the bones, without a fracture that measures radiologically more than 10 mm. Separation of the symphysis pubis is a rare pathology associated with childbirth and has an incidence of 1 in 300 to 1 in 30,000 births. It is usually noticed after delivery but can be observed up to six months postpartum. Risk factors associated with this injury include cephalopelvic disproportion, rapid second stage of labor, epidural anesthesia, severe abduction of the thighs during delivery, or previous trauma to the pelvis. Common signs and symptoms include symphyseal pain aggravated by weight-bearing and walking, a waddling gait, pubic tenderness, and a palpable interpubic gap. Treatment for pubic symphysis diastasis is largely conservative, with treatment modalities including pelvic bracing, bed rest, analgesia, physical therapy, and in some severe cases, surgery.
A GALS screen is an examination used by doctors and other healthcare professionals to detect locomotor abnormalities and functional disability relating to gait, arms, legs and the spine.
Lameness is an abnormal gait or stance of an animal that is the result of dysfunction of the locomotor system. In the horse, it is most commonly caused by pain, but can be due to neurologic or mechanical dysfunction. Lameness is a common veterinary problem in racehorses, sport horses, and pleasure horses. It is one of the most costly health problems for the equine industry, both monetarily for the cost of diagnosis and treatment, and for the cost of time off resulting in loss-of-use.
Scissor gait is a form of gait abnormality primarily associated with spastic cerebral palsy. That condition and others like it are associated with an upper motor neuron lesion.
The Trendelenburg Test or Brodie–Trendelenburg test is a test which can be carried out as part of a physical examination to determine the competency of the valves in the superficial and deep veins of the legs in patients with varicose veins.

The Thomas test is a physical examination test, named after the Welsh orthopaedic surgeon, Hugh Owen Thomas (1834–1891), to rule out hip flexion contracture and psoas syndrome.
Ober's test is used in physical examination to identify tightness of the iliotibial band . During the test, the patient lies on his/her side with the unaffected leg on the bottom with their shoulder and pelvis in line. The lower hip and knee can be in a flexed position to take out any lordosis of the lumbar spine.

Orthotics is a medical specialty that focuses on the design and application of orthoses. An orthosis is "an externally applied device used to influence the structural and functional characteristics of the neuromuscular and skeletal system".

The neuromechanics of idiopathic scoliosis is about the changes in the bones, muscles and joints in cases of spinal deformity consisting of a lateral curvature scoliosis and a rotation of the vertebrae within the curve, that is not explained by either congenital vertebral abnormalities, or neuromuscular disorders such as muscular dystrophy. The idiopathic scoliosis accounts for 80–90% of scoliosis cases. Its pathogenesis is unknown. However, changes in the vestibular system, a lateral shift of the hand representation and abnormal variability of erector spinae motor map location in the motor cortex may be involved in this disease. A short spinal cord and associated nerve tensions has been proposed as a cause and model for idiopathic scoliosis. Besides idiopathic scoliosis being more frequent in certain families, it is suspected to be transmitted via autosomal dominant inheritance. Estrogens could also play a crucial part in the progression of idiopathic scoliosis through their roles in bone formation, growth, maturation and turnover. Finally, collagen, intervertebral disc and muscle abnormalities have been suggested as the cause in idiopathic scoliosis, although these are perhaps results rather than causes.

Gait deviations are nominally referred to as any variation of standard human gait, typically manifesting as a coping mechanism in response to an anatomical impairment. Lower-limb amputees are unable to maintain the characteristic walking patterns of an able-bodied individual due to the removal of some portion of the impaired leg. Without the anatomical structure and neuromechanical control of the removed leg segment, amputees must use alternative compensatory strategies to walk efficiently. Prosthetic limbs provide support to the user and more advanced models attempt to mimic the function of the missing anatomy, including biomechanically controlled ankle and knee joints. However, amputees still display quantifiable differences in many measures of ambulation when compared to able-bodied individuals. Several common observations are whole-body movements, slower and wider steps, shorter strides, and increased sway.