| Hypergammaglobulinemia | |
|---|---|
| Specialty | Immunology, hematology |
Hypergammaglobulinemia is a medical condition with elevated levels of gamma globulin. It is a type of immunoproliferative disorder.
| Hypergammaglobulinemia | |
|---|---|
| Specialty | Immunology, hematology |
Hypergammaglobulinemia is a medical condition with elevated levels of gamma globulin. It is a type of immunoproliferative disorder.
Hypergammaglobulinemia is a condition that is characterized by the increased levels of a certain immunoglobulin in the blood serum. [1] The name of the disorder refers to an excess of proteins after serum protein electrophoresis (found in the gammaglobulin region).[ citation needed ]
Most hypergammaglobulinemias are caused by an excess of immunoglobulin M (IgM), because this is the default immunoglobulin type prior to class switching. Some types of hypergammaglobulinemia are actually caused by a deficiency in the other major types of immunoglobulins, which are IgA, IgE and IgG.
There are 5 types of hypergammaglobulinemias associated with hyper IgM. [2]
MeSH considers hyper IgM syndrome to be a form of dysgammaglobulinemia, not a form of hypergammaglobulinemia.
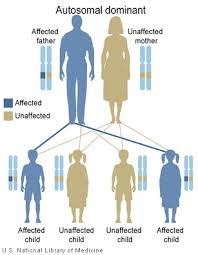
X-linked immunodeficiency with hyper–immunoglobulin M, which is also called type 1 hyper IgM, is a rare form of primary immunodeficiency disease caused by a mutation in the Tumor Necrosis Factor Super Family member 5 (TNFSF5) gene, which codes for CD40 ligand. This gene is located on the long arm of the X chromosome at position 26, denoted Xq26. [3] Normally, CD40 ligand is expressed on activated T cells, and is necessary to induce immunoglobulin class switching from IgM to the other immunoglobulin types. It does this by binding to its ligand, CD40, which is found expressed on the surface of B cells. [4] The mutation in the TNFSF5 gene causes there to be no recognition of CD40 by CD40 ligand, and thus the T cells do not induce Ig class switching in B cells, so there are markedly reduced levels of IgG, IgA, and IgE, but have normal or elevated levels of IgM. CD40 ligand is also required in the functional maturation of T lymphocytes and macrophages, so patients with this disorder have a variable defect in T-lymphocyte and macrophage effector function, as well as hyper IgM. [4]
Immunodeficiency with hyper IgM type 2 is caused by a mutation in the Activation-Induced Cytidine Deaminase (AICDA) gene, which is located on the short arm of chromosome 12. The protein that is encoded by this gene is called Activation-Induced Cytidine Deaminase (AICDA) and functions as a DNA-editing deaminase that induces somatic hypermutation, class switch recombination, and immunoglobulin gene conversion in B cells. [5] When a person is homozygous for the mutation in the AICDA gene, the protein fails to function, and thus somatic hypermutation, class switch recombination, and immunoglobulin gene conversion cannot occur, which creates an excess of IgM. [2]
Immunodeficiency with hyper IgM type 3 is caused by a mutation in the gene that codes for CD40. As mentioned above, CD40 is expressed on the surface of B cells, and its binding to CD40 ligand on activated T cells induces Ig class switching. [4] When the mutation is present, there is no signal for B cells to undergo class switching, so there is an excess of IgM and little to no other immunoglobulin types produced. [2]
Immunodeficiency with hyper IgM type 4 is poorly characterized. All that is known is that there is an excess of IgM in the blood, with normal levels of the other immunoglobulins. The exact cause is yet to be determined. [2]
Immunodeficiency with hyper IgM type 5 is caused by a mutation in the Uracil-DNA glycosylase (UNG) gene, which, like AICDA, is located on chromosome 12. This codes for Uracil DNA Glycosylase, which is responsible for excising previous uracil bases that are due to cytosine deamination, or previous uracil misincorporation from double-stranded previous DNA substrates. This enzyme is also responsible for helping with gene conversion during somatic recombination in B cells. The mutation in the gene causes an enzyme that does not function properly, thus gene conversion does not proceed and class switching cannot occur. [2]

Activation-induced cytidine deaminase, also known as AICDA, AID and single-stranded DNA cytosine deaminase, is a 24 kDa enzyme which in humans is encoded by the AICDA gene. It creates mutations in DNA by deamination of cytosine base, which turns it into uracil. In other words, it changes a C:G base pair into a U:G mismatch. The cell's DNA replication machinery recognizes the U as a T, and hence C:G is converted to a T:A base pair. During germinal center development of B lymphocytes, error-prone DNA repair following AID action also generates other types of mutations, such as C:G to A:T. AID is a member of the APOBEC family.
Hypogammaglobulinemia is an immune system disorder in which not enough gamma globulins are produced in the blood. This results in a lower antibody count, which impairs the immune system, increasing risk of infection. Hypogammaglobulinemia may result from a variety of primary genetic immune system defects, such as common variable immunodeficiency, or it may be caused by secondary effects such as medication, blood cancer, or poor nutrition, or loss of gamma globulins in urine, as in nonselective glomerular proteinuria. Patients with hypogammaglobulinemia have reduced immune function; important considerations include avoiding use of live vaccines, and take precautionary measures when traveling to regions with endemic disease or poor sanitation such as receiving immunizations, taking antibiotics abroad, drinking only safe or boiled water, arranging appropriate medical cover in advance of travel, and ensuring continuation of any immunoglobulin infusions needed.

Cluster of differentiation 40, CD40 is a type I transmembrane protein found on antigen-presenting cells and is required for their activation. The binding of CD154 (CD40L) on TH cells to CD40 activates antigen presenting cells and induces a variety of downstream effects.
In immunology, immunoproliferative disorders are disorders of the immune system that are characterized by the abnormal proliferation of the primary cells of the immune system, which includes B cells, T cells and natural killer (NK) cells, or by the excessive production of immunoglobulins.

Germinal centers or germinal centres (GCs) are transiently formed structures within B cell zone (follicles) in secondary lymphoid organs – lymph nodes, ileal Peyer's patches, and the spleen – where mature B cells are activated, proliferate, differentiate, and mutate their antibody genes during a normal immune response; most of the germinal center B cells (BGC) are removed by tingible body macrophages. There are several key differences between naive B cells and GC B cells, including level of proliferative activity, size, metabolic activity and energy production. The B cells develop dynamically after the activation of follicular B cells by T-dependent antigen. The initiation of germinal center formation involves the interaction between B and T cells in the interfollicular area of the lymph node, CD40-CD40L ligation, NF-kB signaling and expression of IRF4 and BCL6.

CD154, also called CD40 ligand or CD40L, is a protein that is primarily expressed on activated T cells and is a member of the TNF superfamily of molecules. It binds to CD40 on antigen-presenting cells (APC), which leads to many effects depending on the target cell type. In total CD40L has three binding partners: CD40, α5β1 integrin and integrin αIIbβ3. CD154 acts as a costimulatory molecule and is particularly important on a subset of T cells called T follicular helper cells. On TFH cells, CD154 promotes B cell maturation and function by engaging CD40 on the B cell surface and therefore facilitating cell-cell communication. A defect in this gene results in an inability to undergo immunoglobulin class switching and is associated with hyper IgM syndrome. Absence of CD154 also stops the formation of germinal centers and therefore prohibiting antibody affinity maturation, an important process in the adaptive immune system.
Hyper IgM syndrome is a rare primary immune deficiency disorders characterized by low or absent levels of serum IgG, IgA, IgE and normal or increased levels of serum IgM.

Hyper IgM syndrome type 1 (HIGM-1) is the X-linked variant of the hyper IgM syndrome.
Hyper IgM syndrome type 2 is a rare disease. Unlike other hyper-IgM syndromes, type 2 patients identified thus far did not present with a history of opportunistic infections. One would expect opportunistic infections in any immunodeficiency syndrome. The responsible genetic lesion is in the AICDA gene found at 12p13.
The fifth type of hyper-IgM syndrome has been characterized in three patients from France and Japan. The symptoms are similar to hyper IgM syndrome type 2, but the AICDA gene is intact.

Immunoglobulin class switching, also known as isotype switching, isotypic commutation or class-switch recombination (CSR), is a biological mechanism that changes a B cell's production of immunoglobulin from one type to another, such as from the isotype IgM to the isotype IgG. During this process, the constant-region portion of the antibody heavy chain is changed, but the variable region of the heavy chain stays the same. Since the variable region does not change, class switching does not affect antigen specificity. Instead, the antibody retains affinity for the same antigens, but can interact with different effector molecules.
An immune disorder is a dysfunction of the immune system. These disorders can be characterized in several different ways:

IgG deficiency is a form of dysgammaglobulinemia where the proportional levels of the IgG isotype are reduced relative to other immunoglobulin isotypes.
Hyper-IgM syndrome type 3 is a form of hyper IgM syndrome characterized by mutations of the CD40 gene. In this type, Immature B cells cannot receive signal 2 from helper T cells which is necessary to mature into mature B cells.
Hyper-IgM syndrome type 4 is a form of Hyper IgM syndrome which is a defect in class switch recombination downstream of the AICDA gene that does not impair somatic hypermutation.
Somatic hypermutation is a cellular mechanism by which the immune system adapts to the new foreign elements that confront it. A major component of the process of affinity maturation, SHM diversifies B cell receptors used to recognize foreign elements (antigens) and allows the immune system to adapt its response to new threats during the lifetime of an organism. Somatic hypermutation involves a programmed process of mutation affecting the variable regions of immunoglobulin genes. Unlike germline mutation, SHM affects only an organism's individual immune cells, and the mutations are not transmitted to the organism's offspring. Because this mechanism is merely selective and not precisely targeted, somatic hypermutation has been strongly implicated in the development of B-cell lymphomas and many other cancers.
Genome instability refers to a high frequency of mutations within the genome of a cellular lineage. These mutations can include changes in nucleic acid sequences, chromosomal rearrangements or aneuploidy. Genome instability does occur in bacteria. In multicellular organisms genome instability is central to carcinogenesis, and in humans it is also a factor in some neurodegenerative diseases such as amyotrophic lateral sclerosis or the neuromuscular disease myotonic dystrophy.
BENTA disease is a rare genetic disorder of the immune system. BENTA stands for "B cell expansion with NF-κB and T cell anergy" and is caused by germline heterozygous gain-of-function mutations in the gene CARD11. This disorder is characterized by polyclonal B cell lymphocytosis with onset in infancy, splenomegaly, lymphadenopathy, mild immunodeficiency, and increased risk of lymphoma. Investigators Andrew L. Snow and Michael J. Lenardo at the National Institute of Allergy and Infectious Diseases at the U.S. National Institutes of Health first characterized BENTA disease in 2012. Dr. Snow's current laboratory at the Uniformed Services University of the Health Sciences is now actively studying this disorder.

Nina Papavasiliou is an immunologist and Helmholtz Professor in the Division of Immune Diversity at the German Cancer Research Center in Heidelberg, Germany. She is also an adjunct professor at the Rockefeller University, where she was previously associate professor and head of the Laboratory of Lymphocyte Biology. She is best known for her work in the fields of DNA and RNA editing.