Related Research Articles

An antibody (Ab) or immunoglobulin (Ig) is a large, Y-shaped protein belonging to the immunoglobulin superfamily which is used by the immune system to identify and neutralize antigens such as bacteria and viruses, including those that cause disease. Antibodies can recognize virtually any size antigen with diverse chemical compositions from molecules. Each antibody recognizes one or more specific antigens. Antigen literally means "antibody generator", as it is the presence of an antigen that drives the formation of an antigen-specific antibody. Each tip of the "Y" of an antibody contains a paratope that specifically binds to one particular epitope on an antigen, allowing the two molecules to bind together with precision. Using this mechanism, antibodies can effectively "tag" a microbe or an infected cell for attack by other parts of the immune system, or can neutralize it directly.
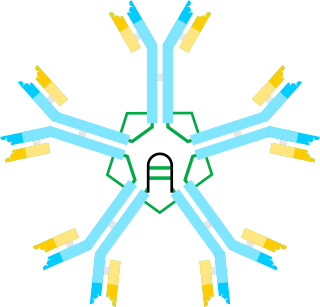
Immunoglobulin M (IgM) is the largest of several isotypes of antibodies that are produced by vertebrates. IgM is the first antibody to appear in the response to initial exposure to an antigen; causing it to also be called an acute phase antibody. In humans and other mammals that have been studied, plasmablasts in the spleen are the main source of specific IgM production.

Cryoglobulinemia is a medical condition in which the blood contains large amounts of pathological cold sensitive antibodies called cryoglobulins – proteins that become insoluble at reduced temperatures. This should be contrasted with cold agglutinins, which cause agglutination of red blood cells.

X-linked agammaglobulinemia (XLA) is a rare genetic disorder discovered in 1952 that affects the body's ability to fight infection. As the form of agammaglobulinemia that is X-linked, it is much more common in males. In people with XLA, the white blood cell formation process does not generate mature B cells, which manifests as a complete or near-complete lack of proteins called gamma globulins, including antibodies, in their bloodstream. B cells are part of the immune system and normally manufacture antibodies, which defend the body from infections by sustaining a humoral immunity response. Patients with untreated XLA are prone to develop serious and even fatal infections. A mutation occurs at the Bruton's tyrosine kinase (Btk) gene that leads to a severe block in B cell development and a reduced immunoglobulin production in the serum. Btk is particularly responsible for mediating B cell development and maturation through a signaling effect on the B cell receptor BCR. Patients typically present in early childhood with recurrent infections, in particular with extracellular, encapsulated bacteria. XLA is deemed to have a relatively low incidence of disease, with an occurrence rate of approximately 1 in 200,000 live births and a frequency of about 1 in 100,000 male newborns. It has no ethnic predisposition. XLA is treated by infusion of human antibody. Treatment with pooled gamma globulin cannot restore a functional population of B cells, but it is sufficient to reduce the severity and number of infections due to the passive immunity granted by the exogenous antibodies.
Hypogammaglobulinemia is an immune system disorder in which not enough gamma globulins are produced in the blood. This results in a lower antibody count, which impairs the immune system, increasing risk of infection. Hypogammaglobulinemia may result from a variety of primary genetic immune system defects, such as common variable immunodeficiency, or it may be caused by secondary effects such as medication, blood cancer, or poor nutrition, or loss of gamma globulins in urine, as in nonselective glomerular proteinuria. Patients with hypogammaglobulinemia have reduced immune function; important considerations include avoiding use of live vaccines, and take precautionary measures when traveling to regions with endemic disease or poor sanitation such as receiving immunizations, taking antibiotics abroad, drinking only safe or boiled water, arranging appropriate medical cover in advance of travel, and ensuring continuation of any immunoglobulin infusions needed.

The immunoglobulin heavy chain (IgH) is the large polypeptide subunit of an antibody (immunoglobulin). In human genome, the IgH gene loci are on chromosome 14.

Monoclonal gammopathy, also known as paraproteinemia, is the presence of excessive amounts of myeloma protein or monoclonal gamma globulin in the blood. It is usually due to an underlying immunoproliferative disorder or hematologic neoplasms, especially multiple myeloma. It is sometimes considered equivalent to plasma cell dyscrasia. The most common form of the disease is monoclonal gammopathy of undetermined significance.

Immunoglobulin class switching, also known as isotype switching, isotypic commutation or class-switch recombination (CSR), is a biological mechanism that changes a B cell's production of immunoglobulin from one type to another, such as from the isotype IgM to the isotype IgG. During this process, the constant-region portion of the antibody heavy chain is changed, but the variable region of the heavy chain stays the same. Since the variable region does not change, class switching does not affect antigen specificity. Instead, the antibody retains affinity for the same antigens, but can interact with different effector molecules.

In immunology, antibodies are classified into several types called isotypes or classes. The variable (V) regions near the tip of the antibody can differ from molecule to molecule in countless ways, allowing it to specifically target an antigen . In contrast, the constant (C) regions only occur in a few variants, which define the antibody's class. Antibodies of different classes activate distinct effector mechanisms in response to an antigen . They appear at different stages of an immune response, differ in structural features, and in their location around the body.
Angioimmunoblastic T-cell lymphoma is a mature T-cell lymphoma of blood or lymph vessel immunoblasts characterized by a polymorphous lymph node infiltrate showing a marked increase in follicular dendritic cells (FDCs) and high endothelial venules (HEVs) and systemic involvement.
Immunoglobulin heavy locus, also known as IGH, is a region on human chromosome 14 that contains a gene for the heavy chains of human antibodies.
Ig heavy chain V-III region VH26 is a protein that in humans is encoded by the IGHV@ gene.

Ig gamma-3 chain C region is a protein that in humans is encoded by the IGHG3 gene.

Fc fragment of IgA receptor (FCAR) is a human gene that codes for the transmembrane receptor FcαRI, also known as CD89. FcαRI binds the heavy-chain constant region of Immunoglobulin A (IgA) antibodies. FcαRI is present on the cell surface of myeloid lineage cells, including neutrophils, monocytes, macrophages, and eosinophils, though it is notably absent from intestinal macrophages and does not appear on mast cells. FcαRI plays a role in both pro- and anti-inflammatory responses depending on the state of IgA bound. Inside-out signaling primes FcαRI in order for it to bind its ligand, while outside-in signaling caused by ligand binding depends on FcαRI association with the Fc receptor gamma chain.
X-linked lymphoproliferative disease is a lymphoproliferative disorder, usually caused by SH2DIA gene mutations in males. XLP-positive individuals experience immune system deficiencies that render them unable to effectively respond to the Epstein-Barr virus (EBV), a common virus in humans that typically induces mild symptoms or infectious mononucleosis (IM) in patients. There are two currently known variations of the disorder, known as XLP1 and XLP2. XLP1 is estimated to occur in approximately one in every million males, while XLP2 is rarer, estimated to occur in one of every five million males. Due to therapies such as chemotherapy and stem cell transplants, the survival rate of XLP1 has increased dramatically since its discovery in the 1970s.
In hematology, plasma cell dyscrasias are a spectrum of progressively more severe monoclonal gammopathies in which a clone or multiple clones of pre-malignant or malignant plasma cells over-produce and secrete into the blood stream a myeloma protein, i.e. an abnormal monoclonal antibody or portion thereof. The exception to this rule is the disorder termed non-secretory multiple myeloma; this disorder is a form of plasma cell dyscrasia in which no myeloma protein is detected in serum or urine of individuals who have clear evidence of an increase in clonal bone marrow plasma cells and/or evidence of clonal plasma cell-mediated tissue injury. Here, a clone of plasma cells refers to group of plasma cells that are abnormal in that they have an identical genetic identity and therefore are descendants of a single genetically distinct ancestor cell.
Hyper-IgM syndrome type 4 is a form of Hyper IgM syndrome which is a defect in class switch recombination downstream of the AICDA gene that does not impair somatic hypermutation.
Cold autoimmune hemolytic anemia caused by cold-reacting antibodies. Autoantibodies that bind to the erythrocyte membrane leading to premature erythrocyte destruction (hemolysis) characterize autoimmune hemolytic anemia.
Epstein–Barr virus–associated lymphoproliferative diseases are a group of disorders in which one or more types of lymphoid cells, i.e. B cells, T cells, NK cells, and histiocytic-dendritic cells, are infected with the Epstein–Barr virus (EBV). This causes the infected cells to divide excessively, and is associated with the development of various non-cancerous, pre-cancerous, and cancerous lymphoproliferative disorders (LPDs). These LPDs include the well-known disorder occurring during the initial infection with the EBV, infectious mononucleosis, and the large number of subsequent disorders that may occur thereafter. The virus is usually involved in the development and/or progression of these LPDs although in some cases it may be an "innocent" bystander, i.e. present in, but not contributing to, the disease.
References
- ↑ "Heavy Chain Diseases: Plasma Cell Disorders: Merck Manual Home Edition" . Retrieved 2008-02-29.
- ↑ Goossens T, Klein U, Küppers R (1998). "Frequent occurrence of deletions and duplications during somatic hypermutation: Implications for oncogene translocations and heavy chain disease". PNAS. 95 (5): 2463–8. Bibcode:1998PNAS...95.2463G. doi: 10.1073/pnas.95.5.2463 . PMC 19376 . PMID 9482908.
- ↑ Corcos D, Dunda O, Butor C, Cesbron JY, Lorès P, Bucchini D, Jami J (1995). "Pre-B-cell development in the absence of lambda 5 in transgenic mice expressing a heavy-chain disease protein". Curr. Biol. 5 (10): 1140–8. doi: 10.1016/S0960-9822(95)00230-2 . PMID 8548286. S2CID 18737035.
- ↑ Corcos D, Osborn MJ, Matheson LS, Santos F, Zou X, Smith JA, Morgan G, Hutchings A, Hamon M, Oxley D, Brüggemann M (2010). "Immunoglobulin aggregation leading to Russell body formation is prevented by the antibody light chain". Blood. 115 (2): 282–8. doi: 10.1182/blood-2009-07-234864 . PMID 19822901.
- ↑ Fakhfakh F, Dellagi K, Ayadi H, Bouguerra A, Fourati R, Ben Ayed F, Brouet JC, Tsapis A (1992). "Alpha heavy chain disease alpha mRNA contain nucleotide sequences of unknown origins". Eur. J. Immunol. 22 (11): 3037–40. doi:10.1002/eji.1830221141. PMID 1425927. S2CID 85132431.
- 1 2 3 Weng CH, Wang RC, Hsieh TY, Tsai CA, Lin TH (July 2012). "Penicillium pneumonia in a patient with newly diagnosed Franklin disease". Am J Med Sci. 344 (1): 69–71. doi:10.1097/MAJ.0b013e31824a8927. PMID 22543591.
- ↑ Wahner-Roedler DL, Witzig TE, Loehrer LL, Kyle RA (2003). "Gamma-heavy chain disease: review of 23 cases". Medicine (Baltimore). 82 (4): 236–50. doi: 10.1097/01.md.0000085058.63483.7f . PMID 12861101. S2CID 5320931.
- ↑ Wahner-Roedler DL, Kyle RA (1992). "Mu-heavy chain disease: presentation as a benign monoclonal gammopathy". Am. J. Hematol. 40 (1): 56–60. doi:10.1002/ajh.2830400112. PMID 1566748. S2CID 37749139.
- ↑ Vilpo JA, Irjala K, Viljanen MK, Klemi P, Kouvonen I, Rönnemaa T (1980). "Delta-Heavy chain disease: A study of a case". Clin Immunol Immunopathol. 17 (4): 584–94. doi:10.1016/0090-1229(80)90154-3. PMID 6777103.
- 1 2 3 Wahner-Roedler DL, Kyle RA (2005). "Heavy chain diseases". Best Pract Res Clin Haematol. 18 (4): 729–46. doi:10.1016/j.beha.2005.01.029. PMID 16026747.
- 1 2 3 Fermand JP, Brouet JC, Danon F, Seligmann M (1989). "Gamma heavy chain "disease": heterogeneity of the clinicopathologic features. Report of 16 cases and review of the literature". Medicine (Baltimore). 68 (6): 321–35. doi: 10.1097/00005792-198911000-00001 . PMID 2509855. S2CID 29644848.