Related Research Articles

Chronic lymphocytic leukemia (CLL) is a type of cancer in which the bone marrow makes too many lymphocytes. Early on, there are typically no symptoms. Later, non-painful lymph node swelling, feeling tired, fever, night sweats, or weight loss for no clear reason may occur. Enlargement of the spleen and low red blood cells (anemia) may also occur. It typically worsens gradually over years.
Follicular lymphoma (FL) is a cancer that involves certain types of white blood cells known as lymphocytes. The cancer originates from the uncontrolled division of specific types of B-cells known as centrocytes and centroblasts. These cells normally occupy the follicles in the germinal centers of lymphoid tissues such as lymph nodes. The cancerous cells in FL typically form follicular or follicle-like structures in the tissues they invade. These structures are usually the dominant histological feature of this cancer.
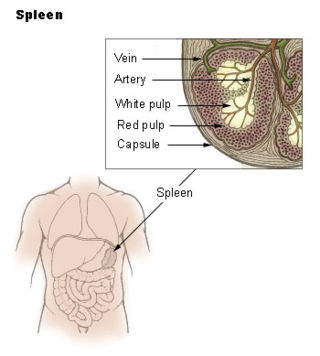
The marginal zone is the region at the interface between the non-lymphoid red pulp and the lymphoid white-pulp of the spleen.
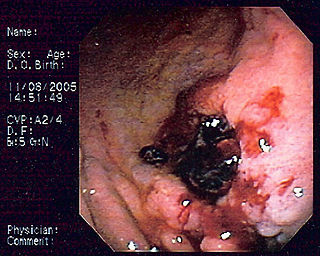
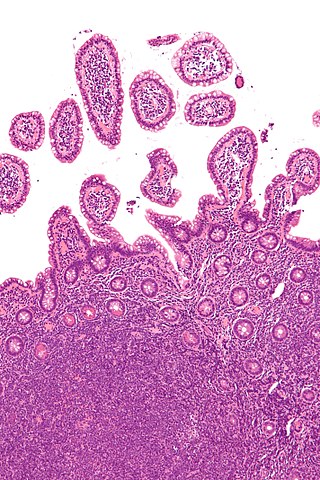
MALT lymphoma is a form of lymphoma involving the mucosa-associated lymphoid tissue (MALT), frequently of the stomach, but virtually any mucosal site can be affected. It is a cancer originating from B cells in the marginal zone of the MALT.
The B-cell lymphomas are types of lymphoma affecting B cells. Lymphomas are "blood cancers" in the lymph nodes. They develop more frequently in older adults and in immunocompromised individuals.
Diffuse large B-cell lymphoma (DLBCL) is a cancer of B cells, a type of lymphocyte that is responsible for producing antibodies. It is the most common form of non-Hodgkin lymphoma among adults, with an annual incidence of 7–8 cases per 100,000 people per year in the US and UK. This cancer occurs primarily in older individuals, with a median age of diagnosis at ~70 years, although it can occur in young adults and, in rare cases, children. DLBCL can arise in virtually any part of the body and, depending on various factors, is often a very aggressive malignancy. The first sign of this illness is typically the observation of a rapidly growing mass or tissue infiltration that is sometimes associated with systemic B symptoms, e.g. fever, weight loss, and night sweats.

T-cell-prolymphocytic leukemia (T-PLL) is a mature T-cell leukemia with aggressive behavior and predilection for blood, bone marrow, lymph nodes, liver, spleen, and skin involvement. T-PLL is a very rare leukemia, primarily affecting adults over the age of 30. It represents 2% of all small lymphocytic leukemias in adults. Other names include T-cell chronic lymphocytic leukemia, "knobby" type of T-cell leukemia, and T-prolymphocytic leukemia/T-cell lymphocytic leukemia.
Large granular lymphocytic (LGL) leukemia is a chronic lymphoproliferative disorder that exhibits an unexplained, chronic elevation in large granular lymphocytes (LGLs) in the peripheral blood.
Hepatosplenic T-cell lymphoma is a rare form of lymphoma that is generally incurable, except in the case of an allogeneic stem cell transplant. It is a systemic neoplasm comprising medium-sized cytotoxic T-cells that show significant sinusoidal infiltration in the liver, spleen, and bone marrow.
Richter's transformation (RT), also known as Richter's syndrome, is the conversion of chronic lymphocytic leukemia (CLL) or its variant, small lymphocytic lymphoma (SLL), into a new and more aggressively malignant disease. CLL is the circulation of malignant B lymphocytes with or without the infiltration of these cells into lymphatic or other tissues while SLL is the infiltration of these malignant B lymphocytes into lymphatic and/or other tissues with little or no circulation of these cells in the blood. CLL along with its SLL variant are grouped together in the term CLL/SLL.
B-cell prolymphocytic leukemia, referred to as B-PLL, is a rare blood cancer. It is a more aggressive, but still treatable, form of leukemia.
Mantle cell lymphoma (MCL) is a type of non-Hodgkin's lymphoma, comprising about 6% of cases. It is named for the mantle zone of the lymph nodes where it develops. The term 'mantle cell lymphoma' was first adopted by Raffeld and Jaffe in 1991.

Marginal zone lymphomas, also known as marginal zone B-cell lymphomas (MZLs), are a heterogeneous group of lymphomas that derive from the malignant transformation of marginal zone B-cells. Marginal zone B cells are innate lymphoid cells that normally function by rapidly mounting IgM antibody immune responses to antigens such as those presented by infectious agents and damaged tissues. They are lymphocytes of the B-cell line that originate and mature in secondary lymphoid follicles and then move to the marginal zones of mucosa-associated lymphoid tissue (MALT), the spleen, or lymph nodes. Mucosa-associated lymphoid tissue is a diffuse system of small concentrations of lymphoid tissue found in various submucosal membrane sites of the body such as the gastrointestinal tract, mouth, nasal cavity, pharynx, thyroid gland, breast, lung, salivary glands, eye, skin and the human spleen.

Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) is a slow-growing CD20 positive form of Hodgkin lymphoma, a cancer of the immune system's B cells.
Monoclonal B-cell lymphocytosis (MBL) is an asymptomatic condition in which individuals have increased blood levels of particular subtypes of monoclonal lymphocytes. This increase must persist for at least 3 months. The lymphocyte subtypes are B-cells that share certain features with the abnormal clones of lymphocytes that circulate in chronic lymphocytic leukemia/small lymphocyte lymphoma (CLL/SLL) or, less frequently, other types of B-cell malignancies. Some individuals with these circulating B-cells develop CLL/SLL or the lymphoma types indicated by their circulating monoclonal B-cells. Hence, MBL is a premalignant disorder
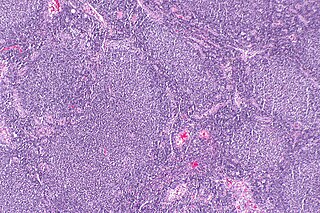
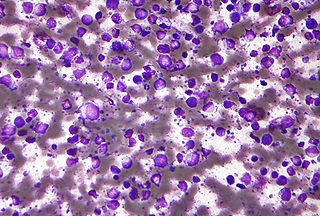
Splenic lymphoma with villous lymphocytes is a rare type of lymphoma that involves mature B cells. Older names include lymphoma simulating hairy cell leukemia and lymphoplasmacytic lymphoma with circulating villous lymphocytes. The characteristic villous lymphocytes will appear in a blood smear of the peripheral blood of patients with this type of lymphoma. These lymphocytes will have an oval nucleus with the “cobblestone” pattern of nuclear chromatin typical of more mature lymphoid cells. The cytoplasmic projections, or villi, are found in a polar distribution. Whether this condition is identical to splenic marginal zone lymphoma, or only highly similar, is a matter of debate.

t(11;14) is a chromosomal translocation which essentially always involves the immunoglobulin heavy locus, also known as IGH in the q32 region of chromosome 14, as well as cyclin D1 which is located in the q13 of chromosome 11. Specifically, the translocation is at t(11;14)(q13;q32).
In situ lymphoid neoplasia is a precancerous condition newly classified by the World Health Organization in 2016. The Organization recognized two subtypes of ISLN: in situ follicular neoplasia (ISFN) and in situ mantle cell neoplasia (ISMCL). ISFN and ISMCL are pathological accumulations of lymphocytes in the germinal centers and mantle zones, respectively, of the follicles that populate lymphoid organs such as lymph nodes. These lymphocytes are monoclonal B-cells that may develop into follicular (FL) and mantle cell (MCL) lymphomas, respectively.
Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) is a cutaneous lymphoma skin disease that occurs mostly in elderly females. In this disease, B cells become malignant, accumulate in the dermis and subcutaneous tissue below the dermis to form red and violaceous skin nodules and tumors. These lesions typically occur on the lower extremities but in uncommon cases may develop on the skin at virtually any other site. In ~10% of cases, the disease presents with one or more skin lesions none of which are on the lower extremities; the disease in these cases is sometimes regarded as a variant of PCDLBL, LT termed primary cutaneous diffuse large B-cell lymphoma, other (PCDLBC-O). PCDLBCL, LT is a subtype of the diffuse large B-cell lymphomas (DLBCL) and has been thought of as a cutaneous counterpart to them. Like most variants and subtypes of the DLBCL, PCDLBCL, LT is an aggressive malignancy. It has a 5-year overall survival rate of 40–55%, although the PCDLBCL-O variant has a better prognosis than cases in which the legs are involved.

Indolent lymphoma, also known as low-grade lymphoma, is a group of slow-growing non-Hodgkin lymphomas (NHLs). Because they spread slowly, they tend to have fewer signs and symptoms when first diagnosed and may not require immediate treatment. Symptoms can include swollen but painless lymph nodes, unexplained fever, and unintended weight loss.
References
- 1 2 3 4 5 6 7 8 Elaine Sarkin Jaffe, Nancy Lee Harris, World Health Organization, International Agency for Research on Cancer, Harald Stein, J.W. Vardiman (2001). Pathology and genetics of tumours of haematopoietic and lymphoid tissues. World Health Organization Classification of Tumors. Vol. 3. Lyon: IARC Press. ISBN 978-92-832-2411-2.
{{cite book}}: CS1 maint: multiple names: authors list (link) - ↑ Isaacson PG, Matutes E, Burke M, Catovsky D (1 December 1994). "The histopathology of splenic lymphoma with villous lymphocytes". Blood. 84 (11): 3828–34. doi: 10.1182/blood.V84.11.3828.bloodjournal84113828 . PMID 7949139.
- ↑ Matutes E, Morilla R, Owusu-Ankomah K, Houlihan A, Catovsky D (15 March 1994). "The immunophenotype of splenic lymphoma with villous lymphocytes and its relevance to the differential diagnosis with other B-cell disorders". Blood. 83 (6): 1558–62. doi: 10.1182/blood.V83.6.1558.1558 . PMID 8123845.
- ↑ Savilo E, Campo E, Mollejo M, et al. (July 1998). "Absence of cyclin D1 protein expression in splenic marginal zone lymphoma". Mod. Pathol. 11 (7): 601–6. PMID 9688179.
- ↑ Dunn-Walters DK, Boursier L, Spencer J, Isaacson PG (June 1998). "Analysis of immunoglobulin genes in splenic marginal zone lymphoma suggests ongoing mutation". Hum. Pathol. 29 (6): 585–93. doi:10.1016/S0046-8177(98)80007-5. PMID 9635678.
- ↑ Corcoran MM, Mould SJ, Orchard JA, et al. (November 1999). "Dysregulation of cyclin dependent kinase 6 expression in splenic marginal zone lymphoma through chromosome 7q translocations". Oncogene. 18 (46): 6271–7. doi: 10.1038/sj.onc.1203033 . PMID 10597225.
- ↑ Franco V, Florena AM, Campesi G (December 1996). "Intrasinusoidal bone marrow infiltration: a possible hallmark of splenic lymphoma". Histopathology. 29 (6): 571–5. doi:10.1046/j.1365-2559.1996.d01-536.x. PMID 8971565. S2CID 37364398.
- ↑ Melo JV, Hegde U, Parreira A, Thompson I, Lampert IA, Catovsky D (June 1987). "Splenic B cell lymphoma with circulating villous lymphocytes: differential diagnosis of B cell leukaemias with large spleens". J. Clin. Pathol. 40 (6): 642–51. doi:10.1136/jcp.40.6.642. PMC 1141055 . PMID 3497180.
- 1 2 Berger F, Felman P, Thieblemont C, et al. (March 2000). "Non-MALT marginal zone B-cell lymphomas: a description of clinical presentation and outcome in 124 patients". Blood. 95 (6): 1950–6. doi:10.1182/blood.V95.6.1950. PMID 10706860.
- 1 2 Mollejo M, Menárguez J, Lloret E, et al. (October 1995). "Splenic marginal zone lymphoma: a distinctive type of low-grade B-cell lymphoma. A clinicopathological study of 13 cases". Am. J. Surg. Pathol. 19 (10): 1146–57. doi:10.1097/00000478-199510000-00005. PMID 7573673.
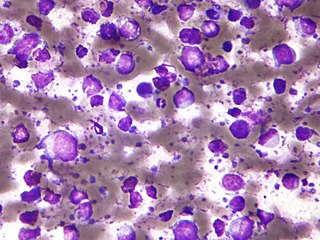
- ↑ Jaffe ES, Costa J, Fauci AS, Cossman J, Tsokos M (November 1983). "Malignant lymphoma and erythrophagocytosis simulating malignant histiocytosis". Am. J. Med. 75 (5): 741–9. doi:10.1016/0002-9343(83)90402-3. PMID 6638043.
- 1 2 3 Arcaini, L. (2006). "Splenic marginal zone lymphoma: a prognostic model for clinical use" (PDF). Blood. 107 (12): 4643–4649. doi:10.1182/blood-2005-11-4659. hdl:11380/584206. ISSN 0006-4971. PMID 16493005. S2CID 13024127.
- ↑ Armitage JO, Weisenburger DD (August 1998). "New approach to classifying non-Hodgkin's lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin's Lymphoma Classification Project". J. Clin. Oncol. 16 (8): 2780–95. doi:10.1200/JCO.1998.16.8.2780. PMID 9704731. Archived from the original on 2013-04-15.