Related Research Articles

Arthroscopy is a minimally invasive surgical procedure on a joint in which an examination and sometimes treatment of damage is performed using an arthroscope, an endoscope that is inserted into the joint through a small incision. Arthroscopic procedures can be performed during ACL reconstruction.
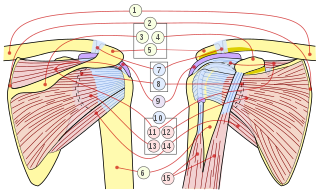
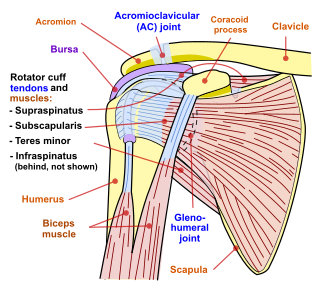
The rotator cuff (SITS muscles) is a group of muscles and their tendons that act to stabilize the human shoulder and allow for its extensive range of motion. Of the seven scapulohumeral muscles, four make up the rotator cuff. The four muscles are:
Shoulder problems including pain, are one of the more common reasons for physician visits for musculoskeletal symptoms. The shoulder is the most movable joint in the body. However, it is an unstable joint because of the range of motion allowed. This instability increases the likelihood of joint injury, often leading to a degenerative process in which tissues break down and no longer function well.

A joint dislocation, also called luxation, occurs when there is an abnormal separation in the joint, where two or more bones meet. A partial dislocation is referred to as a subluxation. Dislocations are often caused by sudden trauma to the joint like an impact or fall. A joint dislocation can cause damage to the surrounding ligaments, tendons, muscles, and nerves. Dislocations can occur in any major joint or minor joint. The most common joint dislocation is a shoulder dislocation.
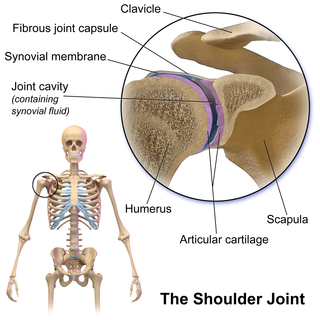
The shoulder joint is structurally classified as a synovial ball-and-socket joint and functionally as a diarthrosis and multiaxial joint. It involves an articulation between the glenoid fossa of the scapula and the head of the humerus. Due to the very loose joint capsule, it gives a limited interface of the humerus and scapula, it is the most mobile joint of the human body.

A SLAP tear or SLAP lesion is an injury to the superior glenoid labrum that initiates in the back of the labrum and stretches toward the front into the attachment point of the long head of the biceps tendon. SLAP is an acronym for "Superior Labrum Anterior and Posterior". SLAP lesions are commonly seen in overhead throwing athletes but middle-aged labor workers can also be affected, and they can be caused by chronic overuse or an acute stretch injury of the shoulder.

The glenoid fossa of the scapula or the glenoid cavity is a bone part of the shoulder. The word glenoid is pronounced or and is from Greek: gléne, "socket", reflecting the shoulder joint's ball-and-socket form. It is a shallow, pyriform articular surface, which is located on the lateral angle of the scapula. It is directed laterally and forward and articulates with the head of the humerus; it is broader below than above and its vertical diameter is the longest.
The glenoid labrum is a fibrocartilaginous structure attached around the rim of the glenoid cavity on the shoulder blade. The shoulder joint is considered a ball-and-socket joint. However, in bony terms the 'socket' is quite shallow and small, covering at most only a third of the 'ball'. The socket is deepened by the glenoid labrum, stabilizing the shoulder joint.
Subacromial bursitis is a condition caused by inflammation of the bursa that separates the superior surface of the supraspinatus tendon from the overlying coraco-acromial ligament, acromion, and coracoid and from the deep surface of the deltoid muscle. The subacromial bursa helps the motion of the supraspinatus tendon of the rotator cuff in activities such as overhead work.

A dislocated shoulder is a condition in which the head of the humerus is detached from the glenoid fossa. Symptoms include shoulder pain and instability. Complications may include a Bankart lesion, Hill-Sachs lesion, rotator cuff tear, or injury to the axillary nerve.
Shoulder surgery is a means of treating injured shoulders. Many surgeries have been developed to repair the muscles, connective tissue, or damaged joints that can arise from traumatic or overuse injuries to the shoulder.
A Bankart lesion is a type of shoulder injury that occurs following a dislocated shoulder. It is an injury of the anterior (inferior) glenoid labrum of the shoulder. When this happens, a pocket at the front of the glenoid forms that allows the humeral head to dislocate into it. It is an indication for surgery and often accompanied by a Hill-Sachs lesion, damage to the posterior humeral head.

A Hill–Sachs lesion, or Hill–Sachs fracture, is a cortical depression in the posterolateral head of the humerus. It results from forceful impaction of the humeral head against the anteroinferior glenoid rim when the shoulder is dislocated anteriorly.

Shoulder replacement is a surgical procedure in which all or part of the glenohumeral joint is replaced by a prosthetic implant. Such joint replacement surgery generally is conducted to relieve arthritis pain or fix severe physical joint damage.
Humeral avulsion of the glenohumeral ligament (HAGL) is defined as an avulsion of the inferior glenohumeral ligament from the anatomic neck of the humerus. In other words, it occurs when we have disruption of the ligaments that join the humerus to the glenoid. HAGL tends to occur in 7.5-9.3% of cases of anterior shoulder instability. Making it an uncommon cause of anterior shoulder instability. Avulsion of this ligamentous complex may occur in three sites: glenoid insertion (40%), the midsubstance (35%) and the humeral insertion (25%). Bony humeral avulsion of the glenohumeral ligament (BHAGL) refers when we have HAGL with bony fracture.

Cunningham shoulder reduction was originally published in 2003 and is an anatomically based method of shoulder reduction that utilizes positioning, voluntary scapular retraction, and bicipital massage. It is designed for true anterior/subcoracoid glenohumeral dislocations in patients who can fully adduct their humerus. This is distinct from anteroinferior / subglenoid glenohumeral dislocations for which alternative techniques should be used. The method is one of several techniques used for shoulder reduction.
Glenolabral articular disruption (GLAD) lesion is a type of shoulder injury. It is difficult to diagnose clinically, and requires surgical repair to correct the damage to the shoulder.
Bryan L. Reuss is an American orthopaedic surgeon. He received a Bachelor of Arts Degree in Biology with distinction from the University of Kansas in 1996 and graduated with honors with an M.D. from the University of Nebraska College of Medicine in 2000. From 2000 to 2005, Dr. Reuss was an Orthopaedic Surgery Resident Physician in the Orlando Regional Healthcare System. In 2004-2005 he was awarded the "Resident of the Year" for Orlando Regional Healthcare chosen from all the hospital system's Resident Doctors. He completed an Orthopaedic Fellowship at the University of Cincinnati/Wellington Orthopaedics and Sports Medicine Fellowship in 2006. In 2010, Dr. Reuss was awarded the Sports Medicine Person of the Year from the Athletic Trainers Association of Florida.
Shoulder reduction is the process of returning the shoulder to its normal position following a shoulder dislocation. Normally, closed reduction, in which the relationship of bone and joint is manipulated externally without surgical intervention, is used. A variety of techniques exist, but some are preferred due to fewer complications or easier execution. In cases where closed reduction is not successful, open (surgical) reduction may be needed. X-rays are often used to confirm success and absence of associated fractures. The arm should be kept in a sling or immobilizer for several days, prior to supervised recovery of motion and strength.

Reverse shoulder replacement is a type of shoulder replacement in which the normal ball and socket relationship of glenohumeral joint is reversed, creating a more stable joint with a fixed fulcrum. This form of shoulder replacement is utilized in situations in which conventional shoulder replacement surgery would lead to poor outcomes and high failure rates.
References
- 1 2 Latarjet, M (1954). "A propos du traitement des luxations re´cidivante de l'e´paule". Lyon Chir. 49: 994–1003.
- 1 2 Young, AA; Maia R; Berhout J; Walch G (March 2011). "Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint". Journal of Shoulder and Elbow Surgery. 20 (2 Suppl): S61-9. doi:10.1016/j.jse.2010.07.022. PMID 21145262.
- ↑ "Latarjet-Bristow Procedures | ShoulderDoc".
- ↑ Edwards, TB; Boulahia A; Walch G (2003). "Radiographic analysis of bone defects in chronic anterior shoulder instability". Arthroscopy. 19 (7): 732–9. doi:10.1016/S0749-8063(03)00684-4. PMID 12966381.
- ↑ Burkhart, SS; De Beer JF (2000). "Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion". Arthroscopy. 16 (7): 677–94. doi:10.1053/jars.2000.17715. PMID 11027751.
- 1 2 3 Burkhart, SS; De Beer JF; Barth JR; Cresswell T; Roberts C; Richards DP (2007). "Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss". Arthroscopy. 23 (10): 1033–41. doi:10.1016/j.arthro.2007.08.009. PMID 17916467.
- ↑ Lafosse, L; Boyle S (2010). "Arthroscopic Latarjet procedure". J Shoulder Elbow Surg. 19 (2 suppl): 2–12. doi:10.1016/j.jse.2009.12.010. PMID 20188263.
- ↑ Gupta, A; Delaney, R; Petkin, K; Lafosse, L (March 2015). "Complications of the Latarjet procedure". Current Reviews in Musculoskeletal Medicine. 8 (1): 59–66. doi:10.1007/s12178-015-9258-y. PMC 4596182 . PMID 25644052.
- ↑ Allain, J; Goutallier D; Glorion C (1998). "Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder". J Bone Joint Surg Am. 80 (6): 841–52. doi:10.2106/00004623-199806000-00008. PMID 9655102. S2CID 11735619.
- ↑ Hovelius, LB; Akermark C; Albrektsson B; Berg E; Körner L; Lundberg B; Wredmark T (1983). "Bristow-Latarjet procedure for recurrent anterior dislocation of the shoulder. A 2–5 year follow-up study on the results of 112 cases". Acta Orthop Scand. 54 (2): 284–90. doi: 10.3109/17453678308996571 . PMID 6846008.
- ↑ Hovelius, L; Sandström B; Sundgren K; Saebö M (2004). "One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: study I—clinical results". J Shoulder Elbow Surg. 13 (5): 509–16. doi:10.1016/j.jse.2004.02.013. PMID 15383806.
- ↑ Walch, G; Boileau P (2000). "Latarjet-Bristow procedure for recurrent anterior instability". Tech Shoulder Elbow Surg. 1 (4): 256–61. doi:10.1097/00132589-200001040-00008.
- ↑ Joshi, M; Young AA; Balestro J-C; Walch G (2013). "The Latarjet-Patte Procedure for Recurrent Anterior Shoulder Instability in Contact Athletes". Clinics in Sports Medicine. 32 (4): 731–9. doi:10.1016/j.csm.2013.07.009. PMID 24079431.
- ↑ Neyton, L; Young A; Dawidziak B; Visona E; Hager JP; Fournier Y; Walch G. (2012). "Surgical treatment of anterior instability in rugby union players: clinical and radiographic results of the Latarjet-Patte procedure with minimum 5-year follow-up". J Shoulder Elbow Surg. 21 (12): 1721–7. doi:10.1016/j.jse.2012.01.023. PMID 22565042.