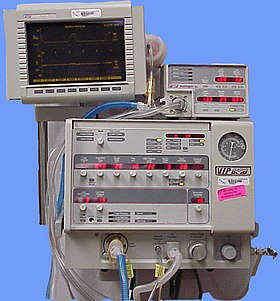
A medical ventilator (or simply ventilator in context) is a machine designed to provide mechanical ventilation by moving breathable air into and out of the lungs, to deliver breaths to a patient who is physically unable to breathe, or breathing insufficiently.
Medical ventilators are sometimes colloquially called "respirators", a term stemming from commonly used devices in the 1950s (particularly the "Bird respirator"). However, in the present-day medical field, the word "respirator" refers to a protective face mask and ventilators are never referred to as respirators.[1]
Function
In its simplest form, a modern positive pressure ventilator consists of a compressible air reservoir or turbine, air and oxygen supplies, a set of valves and tubes, and a disposable or reusable "patient circuit". The air reservoir is pneumatically compressed several times a minute to deliver room-air, or in most cases, an air/oxygen mixture to the patient. If a turbine is used, the turbine pushes air through the ventilator, with a flow valve adjusting pressure to meet patient-specific parameters. When over pressure is released, the patient will exhale passively due to the lungs' elasticity, the exhaled air being released usually through a one-way valve within the patient circuit called the patient manifold.
Ventilators may also be equipped with monitoring and alarm systems for patient-related parameters (e.g. pressure, volume, and flow) and ventilator function (e.g. air leakage, power failure, mechanical failure), backup batteries, oxygen tanks, and remote control. The pneumatic system is nowadays often replaced by a computer-controlled turbopump.
Modern ventilators are electronically controlled by a small embedded system to allow exact adaptation of pressure and flow characteristics to an individual patient's needs. Fine-tuned ventilator settings also serve to make ventilation more tolerable and comfortable for the patient. In Canada and the United States, respiratory therapists are responsible for tuning these settings, while biomedical technologists are responsible for the maintenance. In the United Kingdom and Europe the management of the patient's interaction with the ventilator is done by critical care nurses.
The patient circuit usually consists of a set of three durable, yet lightweight plastic tubes, separated by function (e.g. inhaled air, patient pressure, exhaled air). Determined by the type of ventilation needed, the patient-end of the circuit may be either noninvasive or invasive.
Noninvasive methods, such as Continuous positive airway pressure (CPAP) and Non-invasive ventilation, which are adequate for patients who require a ventilator only while sleeping and resting, mainly employ a nasal mask. Invasive methods require intubation, which for long-term ventilator dependence will normally be a tracheotomy cannula, as this is much more comfortable and practical for long-term care than is larynx or nasal intubation.
Life-critical system
Because failure may result in death, mechanical ventilation systems are classified as a life-critical system, and precautions must be taken to ensure that they are highly reliable, including their power-supply.
Mechanical ventilators are therefore carefully designed so that no single point of failure can endanger the patient. They may have manual backup mechanisms to enable hand-driven respiration in the absence of power (such as the mechanical ventilator integrated into an anaesthetic machine). They may also have safety valves, which open to atmosphere in the absence of power to act as an anti-suffocation valve for spontaneous breathing of the patient. Some systems are also equipped with compressed-gas tanks, air compressors, and/or backup batteries to provide ventilation in case of power failure or defective gas supplies, and methods to operate or call for help if their mechanisms or software fail.
History
The history of mechanical ventilation begins with various versions of what was eventually called the iron lung, a form of noninvasive negative pressure ventilator widely used during the polio epidemics of the 20th century after the introduction of the "Drinker respirator" in 1928, improvements introduced by John Haven Emerson in 1931,[2] and the Both respirator in 1937. Other forms of noninvasive ventilators, also used widely for polio patients, include Biphasic Cuirass Ventilation, the rocking bed, and rather primitive positive pressure machines.[2]
In 1949, John Haven Emerson developed a mechanical assister for anaesthesia with the cooperation of the anaesthesia department at Harvard University. Mechanical ventilators began to be used increasingly in anaesthesia and intensive care during the 1950s. Their development was stimulated both by the need to treat polio patients and the increasing use of muscle relaxants during anaesthesia. Relaxant drugs paralyse the patient and improve operating conditions for the surgeon but also paralyse the respiratory muscles.
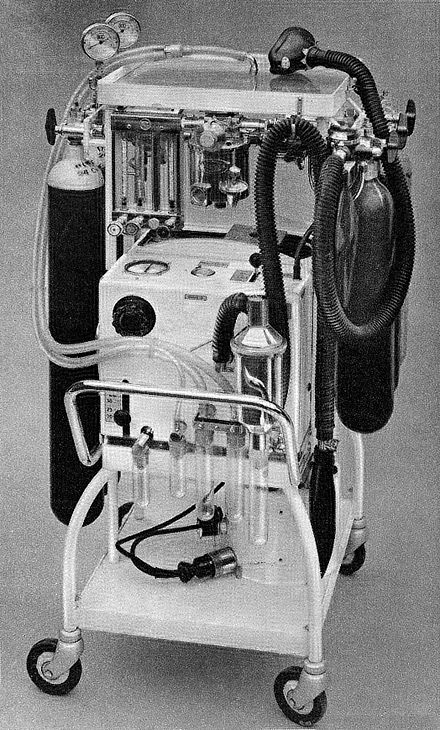
An East-Radcliffe respirator model from the mid-20th century
In the United Kingdom, the East Radcliffe and Beaver models were early examples. The former used a Sturmey-Archer bicycle hub gear to provide a range of speeds, and the latter an automotive windscreen wiper motor to drive the bellows used to inflate the lungs.[3] Electric motors were, however, a problem in the operating theatres of that time, as their use caused an explosion hazard in the presence of flammable anaesthetics such as ether and cyclopropane. In 1952, Roger Manley of the Westminster Hospital, London, developed a ventilator which was entirely gas driven, and became the most popular model used in Europe. It was an elegant design, and became a great favourite with European anaethetists for four decades, prior to the introduction of models controlled by electronics. It was independent of electrical power, and caused no explosion hazard. The original Mark I unit was developed to become the Manley Mark II in collaboration with the Blease company, who manufactured many thousands of these units. Its principle of operation was very simple, an incoming gas flow was used to lift a weighted bellows unit, which fell intermittently under gravity, forcing breathing gases into the patient's lungs. The inflation pressure could be varied by sliding the movable weight on top of the bellows. The volume of gas delivered was adjustable using a curved slider, which restricted bellows excursion. Residual pressure after the completion of expiration was also configurable, using a small weighted arm visible to the lower right of the front panel. This was a robust unit and its availability encouraged the introduction of positive pressure ventilation techniques into mainstream European anesthetic practice.
The 1955 release of Forrest Bird's "Bird Universal Medical Respirator" in the United States changed the way mechanical ventilation was performed, with the small green box becoming a familiar piece of medical equipment.[4] The unit was sold as the Bird Mark 7 Respirator and informally called the "Bird". It was a pneumatic device and therefore required no electrical power source to operate.
In 1965, the Army Emergency Respirator was developed in collaboration with the Harry Diamond Laboratories (now part of the U.S. Army Research Laboratory) and Walter Reed Army Institute of Research. Its design incorporated the principle of fluid amplification in order to govern pneumatic functions. Fluid amplification allowed the respirator to be manufactured entirely without moving parts yet capable of complex resuscitative functions. [5] Elimination of moving parts increased performance reliability and minimized maintenance. [6] The mask is composed of a poly(methyl methacrylate) (also known as lucite) block, about the size of a pack of cards, with machined channels and a cemented and/or screwed-in cover plate. [7] The reduction of moving parts cut manufacturing costs and increased durability. [6]
The bistable fluid amplifier design allowed the respirator to function as both a respiratory assistor and controller. It could functionally transition between assistor and controller automatically based on the patient’s needs. [7][6] The dynamic pressure and turbulent jet flow of gas from inhalation to exhalation allowed the respirator to synchronize with the breathing of the patient. [8]
Intensive care environments around the world revolutionized in 1971 by the introduction of the first SERVO 900 ventilator (Elema-Schönander). It was a small, silent and effective electronic ventilator, with the famous SERVO feedback system controlling what had been set and regulating delivery. For the first time, the machine could deliver the set volume in volume control ventilation.
Ventilators used under increased pressure (hyperbaric) require special precautions and few ventilators can operate under these conditions.[9] In 1979, Sechrist Industries introduced their Model 500A ventilator which was specifically designed for use with hyperbaric chambers.[10]
In 1991 the SERVO 300 ventilator series was introduced. The platform of the SERVO 300 series enabled treatment of all patient categories, from adult to neonate, with one single ventilator. The SERVO 300 series provided a completely new and unique gas delivery system, with rapid flow-triggering response.
In 1999 the LTV (Laptop Ventilator) Series was introduced into the market. The new ventilator was significantly smaller than the ventilators of that time weighing ~14lbs and around the size of a laptop computer. This new design kept the same functionality of the in hospital ventilators, while now opening up a world of opportunity of mobility for the patients.
A modular concept, meaning that the hospital has one ventilator model throughout the ICU department instead of a fleet with different models and brands for the different user needs, was introduced with SERVO-i in 2001. With this modular concept the ICU departments could choose the modes and options, software and hardware needed for a particular patient category.
In the twenty-first century small portable ventilators, for example the SAVe II, have been manufactured for forward combat use. [11]
Mechanical ventilation, or assisted ventilation, is the medical term for artificial ventilation where mechanical means are used to assist or replace spontaneous breathing. This may involve a machine called a ventilator, or the breathing may be assisted manually by a suitably qualified professional, such as an anesthesiologist, Registered Nurse, respiratory therapist, or paramedic, by compressing a bag valve mask device.
A negative pressure ventilator, also known as iron lung (colloquialism) or pulmotor, is a mechanical respirator which enables a person to breathe on his or her own in a normal manner, when muscle control is lost, or the work of breathing exceeds the person's ability. Need for this treatment may result from certain diseases and certain poisons.
Barotrauma is physical damage to body tissues caused by a difference in pressure between a gas space inside, or in contact with, the body, and the surrounding gas or fluid. The initial damage is usually due to over-stretching the tissues in tension or shear, either directly by expansion of the gas in the closed space or by pressure difference hydrostatically transmitted through the tissue. Tissue rupture may be complicated by the introduction of gas into the local tissue or circulation through the initial trauma site, which can cause blockage of circulation at distant sites or interfere with normal function of an organ by its presence.
In physiology, respiration is the movement of oxygen from the outside environment to the cells within tissues, and the transport of carbon dioxide in the opposite direction.
Oxygen therapy, also known as supplemental oxygen, is the use of oxygen as a medical treatment. This can include for low blood oxygen, carbon monoxide toxicity, cluster headaches, and to maintain enough oxygen while inhaled anesthetics are given. Long-term oxygen is often useful in people with chronically low oxygen such as from severe COPD or cystic fibrosis. Oxygen can be given in a number of ways including nasal cannula, face mask, and inside a hyperbaric chamber.
An anaesthetic machine or anesthesia machine is a medical device used to generate and mix a fresh gas flow of medical gases and inhalational anaesthetic agents for the purpose of inducing and maintaining anaesthesia.
Respiratory arrest is caused by apnea or respiratory dysfunction severe enough it will not sustain the body. Prolonged apnea refers to a patient who has stopped breathing for a long period of time. If the heart muscle contraction is intact, the condition is known as respiratory arrest. An abrupt stop of pulmonary gas exchange lasting for more than five minutes may damage vital organs especially the brain, possibly permanently. Lack of oxygen to the brain causes loss of consciousness. Brain injury is likely if respiratory arrest goes untreated for more than three minutes, and death is almost certain if more than five minutes.
Artificial ventilation, is means of assisting or stimulating respiration, a metabolic process referring to the overall exchange of gases in the body by pulmonary ventilation, external respiration, and internal respiration. It may take the form of manually providing air for a person who is not breathing or is not making sufficient respiratory effort, or it may be mechanical ventilation involving the use of a mechanical ventilator to move air in and out of the lungs when an individual is unable to breathe on their own, for example during surgery with general anesthesia or when an individual is in a coma.
A resuscitator is a device using positive pressure to inflate the lungs of an unconscious person who is not breathing, in order to keep them oxygenated and alive. There are three basic types: a manual version consisting of a mask and a large hand-squeezed plastic bulb using ambient air, or with supplemental oxygen from a high-pressure tank. The second type is the Expired Air or breath powered resuscitator. The first appearance of the second type was the Brooke Airway introduced in 1957. The third type is an oxygen powered resuscitator. These are driven by pressurized gas delivered by a regulator, and can either be automatic or manually controlled. The most popular type of gas powered resuscitator are Time Cycled, Volume Constant Ventilators. In the early days of pre-hospital emergency services, pressure cycled devices like the Pulmotor were popular but yielded less than satisfactory results. One of the first modern resuscitation ventilators was the HARV, later called the PneuPac 2R or Yellow Box. Most modern resuscitators are designed to allow the patient to breathe on his own should he recover the ability to do so. All resuscitation devices should be able to deliver >85% oxygen when a gas source is available.
An oxygen mask provides a method to transfer breathing oxygen gas from a storage tank to the lungs. Oxygen masks may cover only the nose and mouth or the entire face. They may be made of plastic, silicone, or rubber.
A bag valve mask (BVM), sometimes known by the proprietary name Ambu bag or generically as a manual resuscitator or "self-inflating bag", is a hand-held device commonly used to provide positive pressure ventilation to patients who are not breathing or not breathing adequately. The device is a required part of resuscitation kits for trained professionals in out-of-hospital settings (such as ambulance crews) and is also frequently used in hospitals as part of standard equipment found on a crash cart, in emergency rooms or other critical care settings. Underscoring the frequency and prominence of BVM use in the United States, the American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiac Care recommend that "all healthcare providers should be familiar with the use of the bag-mask device." Manual resuscitators are also used within the hospital for temporary ventilation of patients dependent on mechanical ventilators when the mechanical ventilator needs to be examined for possible malfunction or when ventilator-dependent patients are transported within the hospital. Two principal types of manual resuscitators exist; one version is self-filling with air, although additional oxygen (O2) can be added but is not necessary for the device to function. The other principal type of manual resuscitator (flow-inflation) is heavily used in non-emergency applications in the operating room to ventilate patients during anesthesia induction and recovery.
High-frequency ventilation is a type of mechanical ventilation which utilizes a respiratory rate greater than four times the normal value. and very small tidal volumes. High frequency ventilation is thought to reduce ventilator-associated lung injury (VALI), especially in the context of ARDS and acute lung injury. This is commonly referred to as lung protective ventilation. There are different types of high-frequency ventilation. Each type has its own unique advantages and disadvantages. The types of HFV are characterized by the delivery system and the type of exhalation phase.
A liquid ventilator is similar to a medical ventilator except that it should be able to ensure reliable total liquid ventilation with a breatheable liquid ·. Liquid ventilators are prototypes that may have been used for animal experimentations but experts recommend continued development of a liquid ventilator toward clinical applications.
An orinasal mask, oro-nasal mask or oral-nasal mask is a breathing mask that covers the mouth and the nose only. It may be a complete independent item, as an oxygen mask, or on some anaesthetic apparatuses, or it may be fitted as a component inside a fullface mask on underwater breathing apparatus, a gas mask or an industrial respirator to reduce the amount of dead space. It may be designed for its lower edge to seal on the front of the lower jaw or to go under the chin.
A breathing tube is a device or tool that can serve as a conduit for breathing. Various types of breathing tubes are available for different specific applications.
Heated humidified high-flow (HHHF) therapy, often also high flow nasal cannula(e) (HFNC) or high flow nasal oxygen (HFNO), is a type of respiratory support method that delivers a high flow of medical gas to a patient through an interface intended to create a wash-out of the upper airway. The applied gas is heated to best match human body temperature and humidified targeting ideal body saturation vapor pressure. It is used in acute and chronic breathing problems.
Modes of mechanical ventilation are one of the most important aspects of the usage of mechanical ventilation. The mode refers to the method of inspiratory support. In general, mode selection is based on clinician familiarity and institutional preferences, since there is a paucity of evidence indicating that the mode affects clinical outcome. The most frequently used forms of volume-limited mechanical ventilation are intermittent mandatory ventilation (IMV) and continuous mandatory ventilation (CMV). There have been substantial changes in the nomenclature of mechanical ventilation over the years, but more recently it has become standardized by many respirology and pulmonology groups. Writing a mode is most proper in all capital letters with a dash between the control variable and the strategy.
Continuous mandatory ventilation (CMV) is a mode of mechanical ventilation in which breaths are delivered based on set variables. Still used in the operating room, in previous nomenclature CMV referred to "controlled mechanical ventilation", a mode of ventilation characterized by a ventilator that makes no effort to sense patient breathing effort. In continuous mandatory ventilation, the ventilator can be triggered either by the patient or mechanically by the ventilator. The ventilator is set to deliver a breath according to parameters selected by the operator. "Controlled mechanical ventilation" is an outdated expansion for "CMV"; "continuous mandatory ventilation" is now accepted standard nomenclature of mechanical ventilation. CMV today can assist or control dynamically, depending on transient presence or absence of spontaneous breathing effort. Thus, today's CMV would have been called ACV in older nomenclature, and the original form of CMV is a thing of the past. But despite continual technological improvement over the past half century, CMV sometimes may still be uncomfortable for the patient.
Many terms are used in mechanical ventilation, some are specific to brand, model, trademark and mode of mechanical ventilation. There is a standardized nomenclature of mechanical ventilation that is specific about nomenclature related to modes, but not settings and variables.
The Bragg-Paul Pulsator, also known as the Bragg-Paul respirator, was a non-invasive medical ventilator invented by William Henry Bragg and designed by Robert W. Paul in 1933 for patients unable to breathe for themselves due to illness.
1 2 Geddes LA (2007). "The history of artificial respiration". IEEE Engineering in Medicine and Biology Magazine. 26 (6): 38–41. doi:10.1109/EMB.2007.907081. PMID18189086.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.