Medical privacy, or health privacy, is the practice of maintaining the security and confidentiality of patient records. It involves both the conversational discretion of health care providers and the security of medical records. The terms can also refer to the physical privacy of patients from other patients and providers while in a medical facility, and to modesty in medical settings. Modern concerns include the degree of disclosure to insurance companies, employers, and other third parties. The advent of electronic medical records (EMR) and patient care management systems (PCMS) have raised new concerns about privacy, balanced with efforts to reduce duplication of services and medical errors.

The Health Insurance Portability and Accountability Act of 1996 is a United States Act of Congress enacted by the 104th United States Congress and signed into law by President Bill Clinton on August 21, 1996. It modernized the flow of healthcare information, stipulates how personally identifiable information maintained by the healthcare and healthcare insurance industries should be protected from fraud and theft, and addressed some limitations on healthcare insurance coverage. It generally prohibits healthcare providers and healthcare businesses, called covered entities, from disclosing protected information to anyone other than a patient and the patient's authorized representatives without their consent. With limited exceptions, it does not restrict patients from receiving information about themselves. It does not prohibit patients from voluntarily sharing their health information however they choose, nor does it require confidentiality where a patient discloses medical information to family members, friends, or other individuals not a part of a covered entity.
A medical error is a preventable adverse effect of care ("iatrogenesis"), whether or not it is evident or harmful to the patient. This might include an inaccurate or incomplete diagnosis or treatment of a disease, injury, syndrome, behavior, infection, or other ailment.
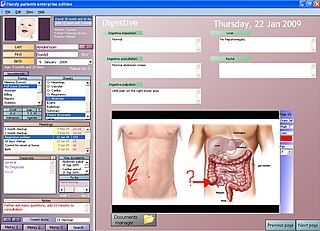
An electronic health record (EHR) is the systematized collection of patient and population electronically stored health information in a digital format. These records can be shared across different health care settings. Records are shared through network-connected, enterprise-wide information systems or other information networks and exchanges. EHRs may include a range of data, including demographics, medical history, medication and allergies, immunization status, laboratory test results, radiology images, vital signs, personal statistics like age and weight, and billing information.
Pharmacovigilance, also known as drug safety, is the pharmaceutical science relating to the "collection, detection, assessment, monitoring, and prevention" of adverse effects with pharmaceutical products. The etymological roots for the word "pharmacovigilance" are: pharmakon and vigilare. As such, pharmacovigilance heavily focuses on adverse drug reactions (ADR), which are defined as any response to a drug which is noxious and unintended, including lack of efficacy. Medication errors such as overdose, and misuse and abuse of a drug as well as drug exposure during pregnancy and breastfeeding, are also of interest, even without an adverse event, because they may result in an adverse drug reaction.
A sentinel event is "any unanticipated event in a healthcare setting that results in death or serious physical or psychological injury to a patient, not related to the natural course of the patient's illness". Sentinel events can be caused by major mistakes and negligence on the part of a healthcare provider, and are closely investigated by healthcare regulatory authorities. Sentinel events are identified under The Joint Commission (TJC) accreditation policies to help aid in root cause analysis and to assist in development of preventive measures. The Joint Commission tracks events in a database to ensure events are adequately analyzed, and that undesirable trends or decreases in performance are caught early and mitigated.
Health technology is defined by the World Health Organization as the "application of organized knowledge and skills in the form of devices, medicines, vaccines, procedures, and systems developed to solve a health problem and improve quality of lives". This includes pharmaceuticals, devices, procedures, and organizational systems used in the healthcare industry, as well as computer-supported information systems. In the United States, these technologies involve standardized physical objects, as well as traditional and designed social means and methods to treat or care for patients.
Patient safety is a discipline that emphasizes safety in health care through the prevention, reduction, reporting and analysis of error and other types of unnecessary harm that often lead to adverse patient events. The frequency and magnitude of avoidable adverse events, often known as patient safety incidents, experienced by patients was not well known until the 1990s, when multiple countries reported significant numbers of patients harmed and killed by medical errors. Recognizing that healthcare errors impact 1 in every 10 patients around the world, the World Health Organization (WHO) calls patient safety an endemic concern. Indeed, patient safety has emerged as a distinct healthcare discipline supported by an immature yet developing scientific framework. There is a significant transdisciplinary body of theoretical and research literature that informs the science of patient safety with mobile health apps being a growing area of research.
A Patient Safety Organization (PSO) is a group, institution, or association that improves medical care by reducing medical errors. Common functions of patient safety organizations are data collection, analysis, reporting, education, funding, and advocacy. A PSO differs from a Federally designed Patient Safety Organization (PSO), which provides health care providers in the U.S. privilege and confidentiality protections for efforts to improve patient safety and the quality of patient care delivery
Signed into effect on 12 June 2002, the Public Health Security and Bioterrorism Preparedness and Response Act of 2002, (PHSBPRA) was signed by the President, the Department of Health and Human Services (DHHS) and the U.S. Department of Agriculture (USDA).
President of the United States George W. Bush signed the Food and Drug Administration Amendments Act of 2007 (FDAAA) on September 27, 2007. This law reviewed, expanded, and reaffirmed several existing pieces of legislation regulating the FDA. These changes allow the FDA to perform more comprehensive reviews of potential new drugs and devices. It was sponsored by Reps. Joe Barton and Frank Pallone and passed unanimously by the Senate.
Crossing the Quality Chasm: A New Health System for the 21st Century is a report on health care quality in the United States published by the Institute of Medicine (IOM) on March 1, 2001. A follow-up to the frequently cited 1999 IOM patient safety report To Err Is Human: Building a Safer Health System, Crossing the Quality Chasm advocates for a fundamental redesign of the U.S. health care system.
Health information technology (HIT) is health technology, particularly information technology, applied to health and health care. It supports health information management across computerized systems and the secure exchange of health information between consumers, providers, payers, and quality monitors. Based on a 2008 report on a small series of studies conducted at four sites that provide ambulatory care – three U.S. medical centers and one in the Netherlands, the use of electronic health records (EHRs) was viewed as the most promising tool for improving the overall quality, safety and efficiency of the health delivery system.
A glossary of terms used in clinical research.
Global Medical Device Nomenclature (GMDN) is a system of internationally agreed generic descriptors used to identify all medical device products. This nomenclature is a naming system for products which include those used for the diagnosis, prevention, monitoring, treatment or alleviation of disease or injury in humans.
Clinical peer review, also known as medical peer review is the process by which health care professionals, including those in nursing and pharmacy, evaluate each other's clinical performance. A discipline-specific process may be referenced accordingly.
The FDA Adverse Event Reporting System is a computerized information database designed to support the U.S. Food and Drug Administration's (FDA) postmarketing safety surveillance program for all approved drug and therapeutic biologic products. The FDA uses FAERS to monitor for new adverse events and medication errors that might occur with these products. It is a system that measures occasional harms from medications to ascertain whether the risk–benefit ratio is high enough to justify continued use of any particular drug and to identify correctable and preventable problems in health care delivery. The system interacts with several related systems including MedWatch and the Vaccine Adverse Event Reporting System. FAERS replaced legacy AERS system in Sep 2012.
The Reagan-Udall Foundation for the Food and Drug Administration is a private nonprofit (501c3) organization, created to support the mission of the U.S. Food and Drug Administration (FDA) to help equip FDA staff with the highest caliber, regulatory science and technology in order to enhance the safety and effectiveness of FDA regulated products. Although it was mandated by Congress in the Food and Drug Administration Amendments Act of 2007 to help support and promote FDA's regulatory science priorities, it is independent of the agency, with its own Board of Directors, staff and research agenda. The Reagan-Udall Foundation creates public–private partnerships to advance research in regulatory science, enhance medical decision making, and promote innovation. It also advances regulatory science through fellowships and other training programs, both for private scientists and for FDA staff.
Health care quality is a level of value provided by any health care resource, as determined by some measurement. As with quality in other fields, it is an assessment of whether something is good enough and whether it is suitable for its purpose. The goal of health care is to provide medical resources of high quality to all who need them; that is, to ensure good quality of life, cure illnesses when possible, to extend life expectancy, and so on. Researchers use a variety of quality measures to attempt to determine health care quality, including counts of a therapy's reduction or lessening of diseases identified by medical diagnosis, a decrease in the number of risk factors which people have following preventive care, or a survey of health indicators in a population who are accessing certain kinds of care.
Privacy in education refers to the broad area of ideologies, practices, and legislation that involve the privacy rights of individuals in the education system. Concepts that are commonly associated with privacy in education include the expectation of privacy, the Family Educational Rights and Privacy Act (FERPA), the Fourth Amendment, and the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Most privacy in education concerns relate to the protection of student data and the privacy of medical records. Many scholars are engaging in an academic discussion that covers the scope of students’ privacy rights, from student in K-12 and even higher education, and the management of student data in an age of rapid access and dissemination of information.

