Related Research Articles
Cosmetic dentistry is generally used to refer to any dental work that improves the appearance of teeth, gums and/or bite. It primarily focuses on improvement in dental aesthetics in color, position, shape, size, alignment and overall smile appearance. Many dentists refer to themselves as "cosmetic dentists" regardless of their specific education, specialty, training, and experience in this field. This has been considered unethical with a predominant objective of marketing to patients. The American Dental Association does not recognize cosmetic dentistry as a formal specialty area of dentistry. However, there are still dentists that promote themselves as cosmetic dentists.

Dental surgery is any of a number of medical procedures that involve artificially modifying dentition; in other words, surgery of the teeth, gums and jaw bones.

A bridge is a fixed dental restoration used to replace one or more missing teeth by joining an artificial tooth definitively to adjacent teeth or dental implants.
Dental restoration, dental fillings, or simply fillings are treatments used to restore the function, integrity, and morphology of missing tooth structure resulting from caries or external trauma as well as to the replacement of such structure supported by dental implants. They are of two broad types—direct and indirect—and are further classified by location and size. A root canal filling, for example, is a restorative technique used to fill the space where the dental pulp normally resides.

A dental technologist is a member of the dental team who, upon prescription from a dental clinician, constructs custom-made restorative and dental appliances.

A dental implant is a prosthesis that interfaces with the bone of the jaw or skull to support a dental prosthesis such as a crown, bridge, denture, or facial prosthesis or to act as an orthodontic anchor. The basis for modern dental implants is a biologic process called osseointegration, in which materials such as titanium or zirconia form an intimate bond to bone. The implant fixture is first placed so that it is likely to osseointegrate, then a dental prosthetic is added. A variable amount of healing time is required for osseointegration before either the dental prosthetic is attached to the implant or an abutment is placed which will hold a dental prosthetic/crown.

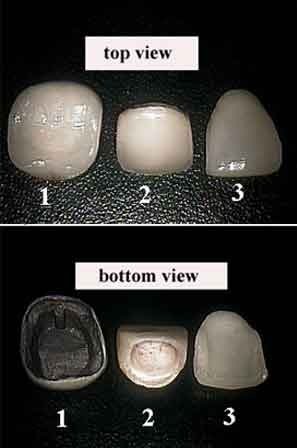
In dentistry, a crown most commonly refers to a dental cap, a type of dental restoration that completely caps or encircles a tooth or dental implant. A crown may be needed when a large cavity threatens the health of a tooth. A crown is typically bonded to the tooth by dental cement. They can be made from various materials, which are usually fabricated using indirect methods. Crowns are used to improve the strength or appearance of teeth and to halt deterioration. While beneficial to dental health, the procedure and materials can be costly.

In dentistry, inlays and onlays are used to fill cavities, and then cemented in place in the tooth. This is an alternative to a direct restoration, made out of composite, amalgam or glass ionomer, that is built up within the mouth.
A removable partial denture (RPD) is a denture for a partially edentulous patient who desires to have replacement teeth for functional or aesthetic reasons and who cannot have a bridge for any reason, such as a lack of required teeth to serve as support for a bridge or financial limitations.
In dentistry, a veneer is a layer of material placed over a tooth. Veneers can improve the aesthetics of a smile and protect the tooth's surface from damage.

A temporary crown is a temporary (short-term) crown used in dentistry. Like other interim restorations, it serves until a final (definitive) restoration can be inserted. Usually the temporary crown is constructed from acrylic resins (monomethacrylate-based/polymethacrylate-based) or, chemical-cure/light cure composite (dimethacrylate-based), although alternative systems using aluminium crown forms are occasionally used. Temporary crowns function to protect the tooth, prevent teeth shifting, provide cosmetics, shape the gum tissue properly, and prevent sensitivity.
A luting agent is an application of a dental cement connecting the underlying tooth structure to a fixed prosthesis. To lute means to glue two different structures together. There are two major purposes of luting agents in dentistry – to secure a cast restoration in fixed prosthodontics, and to keep orthodontic bands and appliances in situ.

CAD/CAM dentistry is a field of dentistry and prosthodontics using CAD/CAM to improve the design and creation of dental restorations, especially dental prostheses, including crowns, crown lays, veneers, inlays and onlays, fixed dental prostheses bridges, dental implant supported restorations, dentures, and orthodontic appliances. CAD/CAM technology allows the delivery of a well-fitting, aesthetic, and a durable prostheses for the patient. CAD/CAM complements earlier technologies used for these purposes by any combination of increasing the speed of design and creation; increasing the convenience or simplicity of the design, creation, and insertion processes; and making possible restorations and appliances that otherwise would have been infeasible. Other goals include reducing unit cost and making affordable restorations and appliances that otherwise would have been prohibitively expensive. However, to date, chairside CAD/CAM often involves extra time on the part of the dentist, and the fee is often at least two times higher than for conventional restorative treatments using lab services.
Fixed prosthodontics is the area of prosthodontics focused on permanently attached (fixed) dental prostheses. Such dental restorations, also referred to as indirect restorations, include crowns, bridges, inlays, onlays, and veneers. Prosthodontists are specialist dentists who have undertaken training recognized by academic institutions in this field. Fixed prosthodontics can be used to restore single or multiple teeth, spanning areas where teeth have been lost. In general, the main advantages of fixed prosthodontics when compared to direct restorations is the superior strength when used in large restorations, and the ability to create an aesthetic looking tooth. As with any dental restoration, principles used to determine the appropriate restoration involves consideration of the materials to be used, extent of tooth destruction, orientation and location of tooth, and condition of neighboring teeth.
A post and core crown is a type of dental restoration required where there is an inadequate amount of sound tooth tissue remaining to retain a conventional crown. A post is cemented into a prepared root canal, which retains a core restoration, which retains the final crown.
A Rochette bridge is a type of dental prosthesis popular in the 1970s, and described by Alain Rochette in 1973 as a form of resin retained bridge that relied on countersunk holes perforating the metal abutment wing. These would be filled with composite cement on seating the restoration, providing macromechanical retention for the prosthesis.
Dental cements have a wide range of dental and orthodontic applications. Common uses include temporary restoration of teeth, cavity linings to provide pulpal protection, sedation or insulation and cementing fixed prosthodontic appliances. Recent uses of dental cement also include two-photon calcium imaging of neuronal activity in brains of animal models in basic experimental neuroscience.

Cracked tooth syndrome (CTS) is where a tooth has incompletely cracked but no part of the tooth has yet broken off. Sometimes it is described as a greenstick fracture. The symptoms are very variable, making it a notoriously difficult condition to diagnose.

Tooth mobility is the horizontal or vertical displacement of a tooth beyond its normal physiological boundaries around the gingival area, i.e. the medical term for a loose tooth.

Overdenture is any removable dental prosthesis that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and/or dental implants. It is one of the most practical measures used in preventive dentistry. Overdentures can be either tooth supported or implant supported. It is found to help in the preservation of alveolar bone and delay the process of complete edentulism.
References
- ↑ Durey, K. A.; Nixon, P. J.; Robinson, S.; Chan, M. F. W.-Y. (2011-08-12). "Resin bonded bridges: techniques for success". British Dental Journal. 211 (3): 113–118. doi: 10.1038/sj.bdj.2011.619 . ISSN 1476-5373. PMID 21836574.
- 1 2 3 Balasubramaniam, G. R. (2017-06-09). "Predictability of resin bonded bridges - a systematic review". British Dental Journal. 222 (11): 849–858. doi:10.1038/sj.bdj.2017.497. ISSN 1476-5373. PMID 28703151.
- 1 2 3 Ibbetson, Richard (2018). "A Contemporary Approach to the Provision of Tooth-Supported Fixed Prostheses Part 1: Indications for Tooth Replacement and the Use of Fixed Bridges Retained by Crowns". Dental Update. 45: 10–20.
- ↑ King PA, Foster LV, Yates RJ, Newcombe RG, Garrett MJ. Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015 Apr 10;218(7):423-8; discussion 428.
- 1 2 3 4 Miettinen, M.; Millar, B. J. (July 2013). "A review of the success and failure characteristics of resin-bonded bridges". British Dental Journal. 215 (2): E3. doi: 10.1038/sj.bdj.2013.686 . ISSN 1476-5373. PMID 23887555.
- ↑ A. Damien Walmsley, Trevor F.Walsh, Phillip J. Lumley, F.J Trevor Burke, Adrian C. Shortall, Richard Hayes-hall, Iain A. Pretty. Restorative Dentistry second edition, Churchill Livingstone, 2007