Related Research Articles
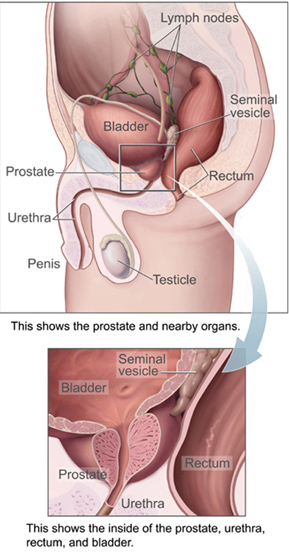
The prostate is both an accessory gland of the male reproductive system and a muscle-driven mechanical switch between urination and ejaculation. It is found in all male mammals. It differs between species anatomically, chemically, and physiologically. Anatomically, the prostate is found below the bladder, with the urethra passing through it. It is described in gross anatomy as consisting of lobes and in microanatomy by zone. It is surrounded by an elastic, fibromuscular capsule and contains glandular tissue, as well as connective tissue.

Prostate cancer is the uncontrolled growth of cells in the prostate, a gland in the male reproductive system just below the bladder. Early prostate cancer usually causes no symptoms. As the tumor grows, it can damage nearby organs causing erectile dysfunction, blood in the urine or semen, and trouble urinating. Some tumors eventually spread to other areas of the body, particularly the bones and lymph nodes. There, tumors cause severe bone pain, leg weakness or paralysis, and eventually death.

Prostate-specific antigen (PSA), also known as gamma-seminoprotein or kallikrein-3 (KLK3), P-30 antigen, is a glycoprotein enzyme encoded in humans by the KLK3 gene. PSA is a member of the kallikrein-related peptidase family and is secreted by the epithelial cells of the prostate gland.

A biopsy is a medical test commonly performed by a surgeon, interventional radiologist, or an interventional cardiologist. The process involves extraction of sample cells or tissues for examination to determine the presence or extent of a disease. The tissue is then fixed, dehydrated, embedded, sectioned, stained and mounted before it is generally examined under a microscope by a pathologist; it may also be analyzed chemically. When an entire lump or suspicious area is removed, the procedure is called an excisional biopsy. An incisional biopsy or core biopsy samples a portion of the abnormal tissue without attempting to remove the entire lesion or tumor. When a sample of tissue or fluid is removed with a needle in such a way that cells are removed without preserving the histological architecture of the tissue cells, the procedure is called a needle aspiration biopsy. Biopsies are most commonly performed for insight into possible cancerous or inflammatory conditions.

Digital rectal examination (DRE), also known as a prostate exam, is an internal examination of the rectum performed by a healthcare provider.

A rectal prolapse occurs when walls of the rectum have prolapsed to such a degree that they protrude out of the anus and are visible outside the body. However, most researchers agree that there are 3 to 5 different types of rectal prolapse, depending on whether the prolapsed section is visible externally, and whether the full or only partial thickness of the rectal wall is involved.
Proctitis is an inflammation of the anus and the lining of the rectum, affecting only the last 6 inches of the rectum.

Prostatectomy is the surgical removal of all or part of the prostate gland. This operation is done for benign conditions that cause urinary retention, as well as for prostate cancer and for other cancers of the pelvis.

Prostate biopsy is a procedure in which small hollow needle-core samples are removed from a man's prostate gland to be examined for the presence of prostate cancer. It is typically performed when the result from a PSA blood test is high. It may also be considered advisable after a digital rectal exam (DRE) finds possible abnormality. PSA screening is controversial as PSA may become elevated due to non-cancerous conditions such as benign prostatic hyperplasia (BPH), by infection, or by manipulation of the prostate during surgery or catheterization. Additionally many prostate cancers detected by screening develop so slowly that they would not cause problems during a man's lifetime, making the complications due to treatment unnecessary.

Pelvic exenteration is a radical surgical treatment that removes all organs from a person's pelvic cavity. It is used to treat certain advanced or recurrent cancers. The urinary bladder, urethra, rectum, and anus are removed. In women, the vagina, cervix, uterus, Fallopian tubes, ovaries and, in some cases, the vulva are removed. In men, the prostate is removed. The procedure leaves the person with a permanent colostomy and urinary diversion.

Radical retropubic prostatectomy is a surgical procedure in which the prostate gland is removed through an incision in the abdomen. It is most often used to treat individuals who have early prostate cancer. Radical retropubic prostatectomy can be performed under general, spinal, or epidural anesthesia and requires blood transfusion less than one-fifth of the time. Radical retropubic prostatectomy is associated with complications such as urinary incontinence and impotence, but these outcomes are related to a combination of individual patient anatomy, surgical technique, and the experience and skill of the surgeon.
Radical perineal prostatectomy is a surgical procedure wherein the entire prostate gland is removed through an incision in the area between the anus and the scrotum (perineum).
Prostate cancer screening is the screening process used to detect undiagnosed prostate cancer in men without signs or symptoms. When abnormal prostate tissue or cancer is found early, it may be easier to treat and cure, but it is unclear if early detection reduces mortality rates.

High-grade prostatic intraepithelial neoplasia (HGPIN) is an abnormality of prostatic glands and believed to precede the development of prostate adenocarcinoma.
Treatment for prostate cancer may involve active surveillance, surgery, radiation therapy – including brachytherapy and external-beam radiation therapy, proton therapy, high-intensity focused ultrasound (HIFU), cryosurgery, hormonal therapy, chemotherapy, or some combination. Treatments also extend to survivorship based interventions. These interventions are focused on five domains including: physical symptoms, psychological symptoms, surveillance, health promotion and care coordination. However, a published review has found only high levels of evidence for interventions that target physical and psychological symptom management and health promotion, with no reviews of interventions for either care coordination or surveillance. The favored treatment option depends on the stage of the disease, the Gleason score, and the PSA level. Other important factors include the man's age, his general health, and his feelings about potential treatments and their possible side-effects. Because all treatments can have significant side-effects, such as erectile dysfunction and urinary incontinence, treatment discussions often focus on balancing the goals of therapy with the risks of lifestyle alterations.

Active surveillance is a management option for localized prostate cancer that can be offered to appropriate patients who would also be candidates for aggressive local therapies, with the intent to intervene if the disease progresses. Active surveillance should not be confused with watchful waiting, another observational strategy for men that would not be candidates for curative therapy because of a limited life expectancy. Active surveillance offers men with a prostate cancer that is thought to have a low risk of causing harm in the absence of treatment, a chance to delay or avoid aggressive treatment and its associated side effects.While prostate cancer is the most common non cutaneous cancer and second leading cause of cancer-related death in American men, it is conservatively estimated that approximately 100,000 men per year in the United States who would be eligible for conservative treatment through active surveillance, undergo unnecessary treatments. The management of localized prostate cancer is controversial and men with localized disease diagnosed today often undergo treatments with significant side effects that will not improve overall health outcomes. The 2011 NIH State-of-the-Science Conference Statement on the "Role of active surveillance in the management of men with localized prostate cancer" pointed out the many unanswered questions about observational strategies for prostate cancer that require further research and clarification. These included:
Specimen provenance complications (SPCs) result from instances of biopsy specimen transposition, extraneous/foreign cell contamination or misidentification of cells used in clinical or anatomical pathology. If left undetected, SPCs can lead to serious diagnostic mistakes and adverse patient outcomes.
Nigro protocol is the preoperative use of chemotherapy with 5-fluorouracil and mitomycin and medical radiation for squamous cell carcinomas of the anal canal. Success of the preoperative regimen changed the paradigm of anal cancer treatment from surgical to non-surgical and was the advent of definitive chemoradiation being accepted as a standard-of-care for anal squamous cell carcinomas. Larger doses of radiation are used in modern chemoradiotherapy protocols versus the original Nigro protocol radiotherapy dose.
Caroline M. Moore is the first woman to be made a professor of urology in the United Kingdom. She works in the diagnosis and treatment of prostate cancer at University College London.
Hashim U. Ahmed is a British surgeon, medical researcher and author of publications in the field of prostate cancer diagnostics and treatment; his research has contributed to changes in the way men with suspected prostate cancer and men with prostate enlargement are diagnosed and treated. He is Professor and Chair of Urology at Imperial College Healthcare NHS Trust and Consultant Urological Surgeon at both Charing Cross Hospital and BUPA Cromwell Hospital.
References
- ↑ Hudson, P. B.; Finkle, A. L.; Hopkins, J. A.; Sproul, E. E.; Stout, A. P. (1954-07-01). "Prostatic cancer. XI. Early prostatic cancer diagnosed by arbitrary open perineal biopsy among 300 unselected patients". Cancer. 7 (4): 690–703. doi:10.1002/1097-0142(195407)7:4<690::aid-cncr2820070410>3.0.co;2-m. ISSN 0008-543X. PMID 13172685.
- 1 2 3 4 5 6 7 8 9 10 Aronowitz, Robert (2013-10-17). ""Screening" for Prostate Cancer in New York's Skid Row: History and Implications". American Journal of Public Health. 104 (1): 70–76. doi:10.2105/AJPH.2013.301446. ISSN 0090-0036. PMC 3910041 . PMID 24134358.
- 1 2 Totten, Robert S. (2016-11-16). "Some Experiences with Latent Carcinoma of the Prostate". Bulletin of the New York Academy of Medicine. 29 (7): 579–582. ISSN 0028-7091. PMC 1877332 . PMID 13051702.
- ↑ Hudson, P. B. (1953-02-01). "Prostatic cancer. IV. Combined surgical and endocrine management of curable lesions". Surgery, Gynecology & Obstetrics. 96 (2): 233–234. ISSN 0039-6087. PMID 13015376.
- ↑ Wyner, Lawrence M. (2 April 2019). "Artist, Rediscovered: Images and Ethics of Early Prostate Cancer Screening". JAMA. 321 (13): 1236–1238. doi:10.1001/jama.2019.1600. PMID 30938779.
- ↑ Kolata, Gina (2013-10-17). "Decades Later, Condemnation for a Skid Row Cancer Study". The New York Times. ISSN 0362-4331 . Retrieved 2016-11-12.
- ↑ "Skid Row Cancer Study Has Implications for Treatment Today, Penn Researcher Says". news.upenn.edu. Retrieved 2016-11-12.
- ↑ Finkle, Alex L.; Moyers, Thomas G.; Tobenkin, Mark I.; Karg, Sara J. (1959-07-18). "Sexual Potency in Aging Males". Journal of the American Medical Association. 170 (12): 1391. doi:10.1001/jama.1959.03010120027008. ISSN 0002-9955. PMID 13664538.
- ↑ Bendiner, E. (1961). The Bowery Man. New York: Thomas Nelson & Sons. p. 169.