
The carpal bones are the eight small bones that make up the wrist (carpus) that connects the hand to the forearm. The term "carpus" and "carpal" is derived from the Latin carpus and the Greek καρπός (karpós), meaning "wrist". In human anatomy, the main role of the carpal bones is to articulate with the radial and ulnar heads to form a highly mobile condyloid joint, to provide attachments for thenar and hypothenar muscles, and to form part of the rigid carpal tunnel which allows the median nerve and tendons of the anterior forearm muscles to be transmitted to the hand and fingers.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.

In human anatomy, the wrist is variously defined as (1) the carpus or carpal bones, the complex of eight bones forming the proximal skeletal segment of the hand; (2) the wrist joint or radiocarpal joint, the joint between the radius and the carpus and; (3) the anatomical region surrounding the carpus including the distal parts of the bones of the forearm and the proximal parts of the metacarpus or five metacarpal bones and the series of joints between these bones, thus referred to as wrist joints. This region also includes the carpal tunnel, the anatomical snuff box, bracelet lines, the flexor retinaculum, and the extensor retinaculum.

The thenar eminence is the mound formed at the base of the thumb on the palm of the hand by the intrinsic group of muscles of the thumb. The skin overlying this region is the area stimulated when trying to elicit a palmomental reflex. The word thenar comes from Ancient Greek θέναρ (thenar) 'palm of the hand'.
In human anatomy, extensor carpi radialis brevis is a muscle in the forearm that acts to extend and abduct the wrist. It is shorter and thicker than its namesake extensor carpi radialis longus which can be found above the proximal end of the extensor carpi radialis brevis.

Wrist drop is a medical condition in which the wrist and the fingers cannot extend at the metacarpophalangeal joints. The wrist remains partially flexed due to an opposing action of flexor muscles of the forearm. As a result, the extensor muscles in the posterior compartment remain paralyzed.

The upper limbs or upper extremities are the forelimbs of an upright-postured tetrapod vertebrate, extending from the scapulae and clavicles down to and including the digits, including all the musculatures and ligaments involved with the shoulder, elbow, wrist and knuckle joints. In humans, each upper limb is divided into the arm, forearm and hand, and is primarily used for climbing, lifting and manipulating objects.
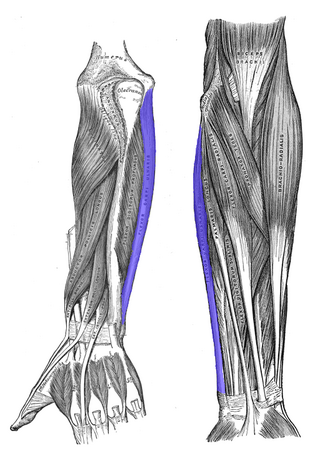
The flexor carpi ulnaris (FCU) is a muscle of the forearm that flexes and adducts at the wrist joint.
In human anatomy, the extensor pollicis longus muscle (EPL) is a skeletal muscle located dorsally on the forearm. It is much larger than the extensor pollicis brevis, the origin of which it partly covers and acts to stretch the thumb together with this muscle.

The flexor pollicis brevis is a muscle in the hand that flexes the thumb. It is one of three thenar muscles. It has both a superficial part and a deep part.
The flexor pollicis longus is a muscle in the forearm and hand that flexes the thumb. It lies in the same plane as the flexor digitorum profundus. This muscle is unique to humans, being either rudimentary or absent in other primates. A meta-analysis indicated accessory flexor pollicis longus is present in around 48% of the population.

In human anatomy, the abductor digiti minimi is a skeletal muscle situated on the ulnar border of the palm of the hand. It forms the ulnar border of the palm and its spindle-like shape defines the hypothenar eminence of the palm together with the skin, connective tissue, and fat surrounding it. Its main function is to pull the little finger away from the other fingers.
The flexor retinaculum is a fibrous band on the palmar side of the hand near the wrist. It arches over the carpal bones of the hands, covering them and forming the carpal tunnel.

The extensor retinaculum is a thickened portion of the antebrachial fascia that holds the tendons of the extensor muscles in place. It is located on the back of the forearm, just proximal to the hand. It is continuous with the palmar carpal ligament.

In the human body, the carpal tunnel or carpal canal is a flattened body cavity on the flexor (palmar/volar) side of the wrist, bounded by the carpal bones and flexor retinaculum. It forms the passageway that transmits the median nerve and the tendons of the extrinsic flexor muscles of the hand from the forearm to the hand. There are described cases of the anatomical variant median artery occurrence.
Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.

The extrinsic extensor muscles of the hand are located in the back of the forearm and have long tendons connecting them to bones in the hand, where they exert their action. Extrinsic denotes their location outside the hand. Extensor denotes their action which is to extend, or open flat, joints in the hand. They include the extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor digitorum (ED), extensor digiti minimi (EDM), extensor carpi ulnaris (ECU), abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor pollicis longus (EPL), and extensor indicis (EI).

The muscles of the thumb are nine skeletal muscles located in the hand and forearm. The muscles allow for flexion, extension, adduction, abduction and opposition of the thumb. The muscles acting on the thumb can be divided into two groups: The extrinsic hand muscles, with their muscle bellies located in the forearm, and the intrinsic hand muscles, with their muscles bellies located in the hand proper.
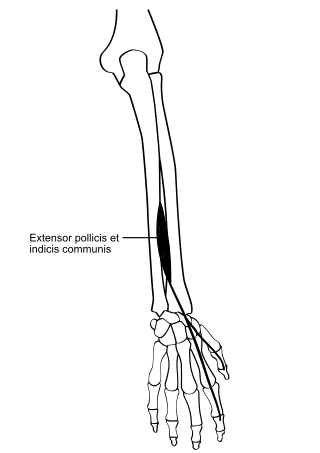
In human anatomy, the extensor pollicis et indicis communis is an aberrant muscle in the posterior compartment of forearm. It was first described in 1863. The muscle has a prevalence from 0.5% to 4%.
Linburg–Comstock variation is an occasional tendinous connection between the flexor pollicis longus and the flexor digitorum profundus of the index, the middle finger or both. It is found in around 21% of the population. It is an anatomical variation in human, which may be viewed as a pathology if causes symptoms. It was recognised as early as the 1800s, but was first described by Linburg and Comstock in 1979.


