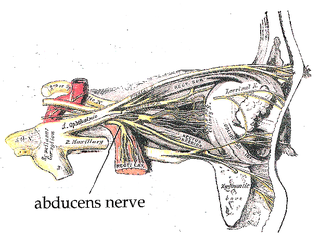
The abducens nerve or abducent nerve, also known as the sixth cranial nerve, cranial nerve VI, or simply CN VI, is a cranial nerve in humans and various other animals that controls the movement of the lateral rectus muscle, one of the extraocular muscles responsible for outward gaze. It is a somatic efferent nerve.
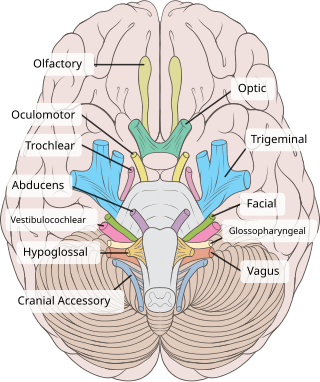
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
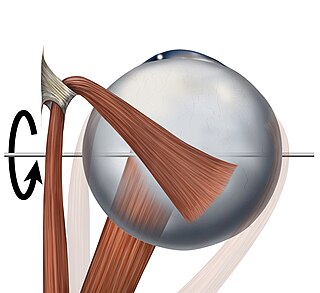
The trochlear nerve, also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye. Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve.

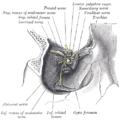
In anatomy, the orbit is the cavity or socket/hole of the skull in which the eye and its appendages are situated. "Orbit" can refer to the bony socket, or it can also be used to imply the contents. In the adult human, the volume of the orbit is 30 millilitres, of which the eye occupies 6.5 ml. The orbital contents comprise the eye, the orbital and retrobulbar fascia, extraocular muscles, cranial nerves II, III, IV, V, and VI, blood vessels, fat, the lacrimal gland with its sac and duct, the eyelids, medial and lateral palpebral ligaments, cheek ligaments, the suspensory ligament, septum, ciliary ganglion and short ciliary nerves.

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.

The superior rectus muscle is a muscle in the orbit. It is one of the extraocular muscles. It is innervated by the superior division of the oculomotor nerve (III). In the primary position, its primary function is elevation, although it also contributes to intorsion and adduction. It is associated with a number of medical conditions, and may be weak, paralysed, overreactive, or even congenitally absent in some people.
The inferior rectus muscle is a muscle in the orbit near the eye. It is one of the four recti muscles in the group of extraocular muscles. It originates from the common tendinous ring, and inserts into the anteroinferior surface of the eye. It depresses the eye (downwards).

The lateral rectus muscle is a muscle on the lateral side of the eye in the orbit. It is one of six extraocular muscles that control the movements of the eye. The lateral rectus muscle is responsible for lateral movement of the eyeball, specifically abduction. Abduction describes the movement of the eye away from the midline, allowing the eyeball to move horizontally in the lateral direction, bringing the pupil away from the midline of the body.
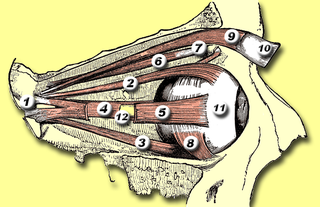
The medial rectus muscle is a muscle in the orbit near the eye. It is one of the extraocular muscles. It originates from the common tendinous ring, and inserts into the anteromedial surface of the eye. It is supplied by the inferior division of the oculomotor nerve (III). It rotates the eye medially (adduction).
The inferior oblique muscle or obliquus oculi inferior is a thin, narrow muscle placed near the anterior margin of the floor of the orbit. The inferior oblique is one of the extraocular muscles, and is attached to the maxillary bone (origin) and the posterior, inferior, lateral surface of the eye (insertion). The inferior oblique is innervated by the inferior branch of the oculomotor nerve.

The extraocular muscles, or extrinsic ocular muscles, are the seven extrinsic muscles of the eye in humans and other animals. Six of the extraocular muscles, the four recti muscles, and the superior and inferior oblique muscles, control movement of the eye. The other muscle, the levator palpebrae superioris, controls eyelid elevation. The actions of the six muscles responsible for eye movement depend on the position of the eye at the time of muscle contraction.
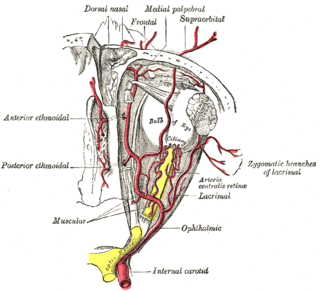
The ophthalmic artery (OA) is an artery of the head. It is the first branch of the internal carotid artery distal to the cavernous sinus. Branches of the ophthalmic artery supply all the structures in the orbit around the eye, as well as some structures in the nose, face, and meninges. Occlusion of the ophthalmic artery or its branches can produce sight-threatening conditions.
The common tendinous ring, also known as the annulus of Zinn or annular tendon, is a ring of fibrous tissue surrounding the optic nerve at its entrance at the apex of the orbit. It is the common origin of the four recti muscles of the group of extraocular muscles.
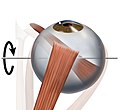
Trochleitis is inflammation of the superior oblique tendon trochlea apparatus characterized by localized swelling, tenderness, and severe pain. This condition is an uncommon but treatable cause of periorbital pain. The trochlea is a ring-like apparatus of cartilage through which passes the tendon of the superior oblique muscle. It is located in the superior nasal orbit and functions as a pulley for the superior oblique muscle. Inflammation of the trochlear region leads to a painful syndrome with swelling and exquisite point tenderness in the upper medial rim of the orbit. A vicious cycle may ensue such that inflammation causes swelling and fraying of the tendon which then increases the friction of passing through the trochlea which in turn adds to the inflammation. Trochleitis has also been associated with triggering or worsening of migraine attacks in patients with pre-existing migraines.

Tenon's capsule, also known as the Tenon capsule, fascial sheath of the eyeball or the fascia bulbi, is a thin membrane which envelops the eyeball from the optic nerve to the corneal limbus, separating it from the orbital fat and forming a socket in which it moves.
The trochlea of superior oblique is a pulley-like structure in the eye. The tendon of the superior oblique muscle passes through it. Situated on the superior nasal aspect of the frontal bone, it is the only cartilage found in the normal orbit. The word trochlea comes from the Greek word for pulley.

The cranial nerve exam is a type of neurological examination. It is used to identify problems with the cranial nerves by physical examination. It has nine components. Each test is designed to assess the status of one or more of the twelve cranial nerves (I-XII). These components correspond to testing the sense of smell (I), visual fields and acuity (II), eye movements and pupils, sensory function of face (V), strength of facial (VII) and shoulder girdle muscles (XI), hearing and balance, taste, pharyngeal movement and reflex, tongue movements (XII).

The following outline is provided as an overview of and topical guide to human anatomy:
The term gaze is frequently used in physiology to describe coordinated motion of the eyes and neck. The lateral gaze is controlled by the paramedian pontine reticular formation (PPRF). The vertical gaze is controlled by the rostral interstitial nucleus of medial longitudinal fasciculus and the interstitial nucleus of Cajal.
The Parks–Bielschowsky three-step test, also known as Park's three-step test or Bielschowsky head tilt test, is a method used to isolate the paretic extraocular muscle, particularly superior oblique muscle and trochlear nerve, in acquired vertical double vision. It was originally described by Marshall M. Parks.