
The leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. The thigh is between the hip and knee, while the calf (rear) and shin (front) are between the knee and foot.

The sciatic nerve, also called the ischiadic nerve, is a large nerve in humans and other vertebrate animals which is the largest branch of the sacral plexus and runs alongside the hip joint and down the lower limb. It is the longest and widest single nerve in the human body, going from the top of the leg to the foot on the posterior aspect. The sciatic nerve has no cutaneous branches for the thigh. This nerve provides the connection to the nervous system for the skin of the lateral leg and the whole foot, the muscles of the back of the thigh, and those of the leg and foot. It is derived from spinal nerves L4 to S3. It contains fibers from both the anterior and posterior divisions of the lumbosacral plexus.

The gluteus medius, one of the three gluteal muscles, is a broad, thick, radiating muscle. It is situated on the outer surface of the pelvis.

The gluteus minimus, or glutæus minimus, the smallest of the three gluteal muscles, is situated immediately beneath the gluteus medius.

The piriformis muscle is a flat, pyramidally-shaped muscle in the gluteal region of the lower limbs. It is one of the six muscles in the lateral rotator group.

The gluteal sulcus is an area of the body of humans and anthropoid apes, described by a horizontal crease formed by the inferior aspect of the buttocks and the posterior upper thigh. The gluteal sulcus is formed by the posterior horizontal skin crease of the hip joint and overlying fat and is not formed by the lower border of the gluteus maximus muscle, which crosses the fold obliquely. It is one of the major defining features of the buttocks. Children with developmental dysplasia of the hips are born with uneven gluteal folds and can be diagnosed with a physical examination and sonogram.
The biceps femoris is a muscle of the thigh located to the posterior, or back. As its name implies, it consists of two heads; the long head is considered part of the hamstring muscle group, while the short head is sometimes excluded from this characterization, as it only causes knee flexion and is activated by a separate nerve.
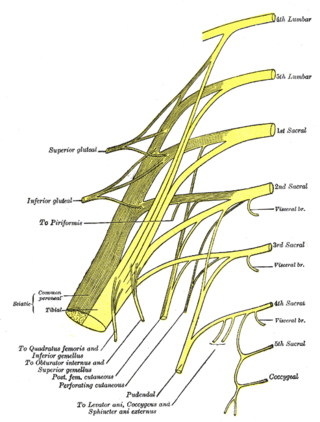
In human anatomy, the sacral plexus is a nerve plexus which provides motor and sensory nerves for the posterior thigh, most of the lower leg and foot, and part of the pelvis. It is part of the lumbosacral plexus and emerges from the lumbar vertebrae and sacral vertebrae (L4-S4). A sacral plexopathy is a disorder affecting the nerves of the sacral plexus, usually caused by trauma, nerve compression, vascular disease, or infection. Symptoms may include pain, loss of motor control, and sensory deficits.

The tensor fasciae latae is a muscle of the thigh. Together with the gluteus maximus, it acts on the iliotibial band and is continuous with the iliotibial tract, which attaches to the tibia. The muscle assists in keeping the balance of the pelvis while standing, walking, or running.

The internal iliac artery is the main artery of the pelvis.

The posterior cutaneous nerve of the thigh is a sensory nerve of the thigh. It is a branch of the sacral plexus. It supplies the skin of the posterior surface of the thigh, leg, buttock, and also the perineum.
The superior gluteal nerve is a mixed nerve of the sacral plexus that originates in the pelvis. It provides motor innervation to the gluteus medius, gluteus minimus, tensor fasciae latae, and piriformis muscles; it also has a cutaneous branch.

The superior gluteal artery is the terminal branch of the posterior division of the internal iliac artery. It exits the pelvis through the greater sciatic foramen before splitting into a superficial branch and a deep branch.
The inferior gluteal artery is a terminal branch of the anterior trunk of the internal iliac artery. It exits the pelvis through the greater sciatic foramen. It is distributed chiefly to the buttock and the back of the thigh.
The nerve to obturator internus is a mixed nerve providing motor innervation to the obturator internus muscle and gemellus superior muscle, and sensory innervation to the hip joint. It is a branch of the sacral plexus. It is one of the group of deep gluteal nerves.
The nerve to quadratus femoris is a nerve of the sacral plexus that provides motor innervation to the quadratus femoris muscle and gemellus inferior muscle, and an articular branch to the hip joint. The nerve leaves the pelvis through the greater sciatic foramen.

The greater sciatic notch is a notch in the ilium, one of the bones that make up the human pelvis. It lies between the posterior inferior iliac spine (above), and the ischial spine (below). The sacrospinous ligament changes this notch into an opening, the greater sciatic foramen.
The posterior compartment of the thigh is one of the fascial compartments that contains the knee flexors and hip extensors known as the hamstring muscles, as well as vascular and nervous elements, particularly the sciatic nerve.

The following outline is provided as an overview of and topical guide to human anatomy:

The hip bone is a large flat bone, constricted in the center and expanded above and below. In some vertebrates it is composed of three parts: the ilium, ischium, and the pubis.

