Cerebrovascular disease includes a variety of medical conditions that affect the blood vessels of the brain and the cerebral circulation. Arteries supplying oxygen and nutrients to the brain are often damaged or deformed in these disorders. The most common presentation of cerebrovascular disease is an ischemic stroke or mini-stroke and sometimes a hemorrhagic stroke. Hypertension is the most important contributing risk factor for stroke and cerebrovascular diseases as it can change the structure of blood vessels and result in atherosclerosis. Atherosclerosis narrows blood vessels in the brain, resulting in decreased cerebral perfusion. Other risk factors that contribute to stroke include smoking and diabetes. Narrowed cerebral arteries can lead to ischemic stroke, but continually elevated blood pressure can also cause tearing of vessels, leading to a hemorrhagic stroke.

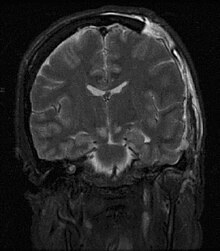
Cerebral edema is excess accumulation of fluid (edema) in the intracellular or extracellular spaces of the brain. This typically causes impaired nerve function, increased pressure within the skull, and can eventually lead to direct compression of brain tissue and blood vessels. Symptoms vary based on the location and extent of edema and generally include headaches, nausea, vomiting, seizures, drowsiness, visual disturbances, dizziness, and in severe cases, death.

Intracranial pressure (ICP) is the pressure exerted by fluids such as cerebrospinal fluid (CSF) inside the skull and on the brain tissue. ICP is measured in millimeters of mercury (mmHg) and at rest, is normally 7–15 mmHg for a supine adult. The body has various mechanisms by which it keeps the ICP stable, with CSF pressures varying by about 1 mmHg in normal adults through shifts in production and absorption of CSF.

Cerebral circulation is the movement of blood through a network of cerebral arteries and veins supplying the brain. The rate of cerebral blood flow in an adult human is typically 750 milliliters per minute, or about 15% of cardiac output. Arteries deliver oxygenated blood, glucose and other nutrients to the brain. Veins carry "used or spent" blood back to the heart, to remove carbon dioxide, lactic acid, and other metabolic products. The neurovascular unit regulates cerebral blood flow so that activated neurons can be supplied with energy in the right amount and at the right time. Because the brain would quickly suffer damage from any stoppage in blood supply, the cerebral circulatory system has safeguards including autoregulation of the blood vessels. The failure of these safeguards may result in a stroke. The volume of blood in circulation is called the cerebral blood flow. Sudden intense accelerations change the gravitational forces perceived by bodies and can severely impair cerebral circulation and normal functions to the point of becoming serious life-threatening conditions.

Intracranial hemorrhage (ICH), also known as intracranial bleed, is bleeding within the skull. Subtypes are intracerebral bleeds, subarachnoid bleeds, epidural bleeds, and subdural bleeds.
Cushing reflex is a physiological nervous system response to increased intracranial pressure (ICP) that results in Cushing's triad of increased blood pressure, irregular breathing, and bradycardia. It is usually seen in the terminal stages of acute head injury and may indicate imminent brain herniation. It can also be seen after the intravenous administration of epinephrine and similar drugs. It was first described in detail by American neurosurgeon Harvey Cushing in 1901.
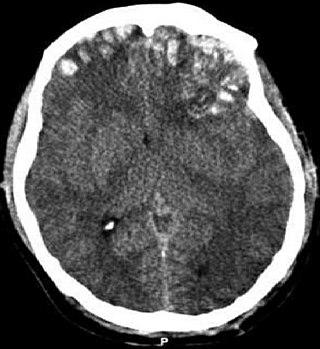
Intracerebral hemorrhage (ICH), also known as hemorrhagic stroke, is a sudden bleeding into the tissues of the brain, into its ventricles, or into both. An ICH is a type of bleeding within the skull and one kind of stroke. Symptoms can vary dramatically depending on the severity, acuity, and location (anatomically) but can include headache, one-sided weakness, numbness, tingling, or paralysis, speech problems, vision or hearing problems, memory loss, attention problems, coordination problems, balance problems, dizziness or lightheadedness or vertigo, nausea/vomiting, seizures, decreased level of consciousness or total loss of consciousness, neck stiffness, and fever.
Cerebral contusion, Latin: contusio cerebri, a form of traumatic brain injury, is a bruise of the brain tissue. Like bruises in other tissues, cerebral contusion can be associated with multiple microhemorrhages, small blood vessel leaks into brain tissue. Contusion occurs in 20–30% of severe head injuries. A cerebral laceration is a similar injury except that, according to their respective definitions, the pia-arachnoid membranes are torn over the site of injury in laceration and are not torn in contusion. The injury can cause a decline in mental function in the long term and in the emergency setting may result in brain herniation, a life-threatening condition in which parts of the brain are squeezed past parts of the skull. Thus treatment aims to prevent dangerous rises in intracranial pressure, the pressure within the skull.
Cerebral perfusion pressure, or CPP, is the net pressure gradient causing cerebral blood flow to the brain. It must be maintained within narrow limits because too little pressure could cause brain tissue to become ischemic, and too much could raise intracranial pressure (ICP).

Decompressive craniectomy is a neurosurgical procedure in which part of the skull is removed to allow a swelling or herniating brain room to expand without being squeezed. It is performed on victims of traumatic brain injury, stroke, Chiari malformation, and other conditions associated with raised intracranial pressure. Use of this surgery is controversial.

Osmotherapy is the use of osmotically active substances to reduce the volume of intracranial contents. Osmotherapy serves as the primary medical treatment for cerebral edema. The primary purpose of osmotherapy is to improve elasticity and decrease intracranial volume by removing free water, accumulated as a result of cerebral edema, from brain's extracellular and intracellular space into vascular compartment by creating an osmotic gradient between the blood and brain. Normal serum osmolality ranges from 280 to 290 mOsm/kg and serum osmolality to cause water removal from brain without much side effects ranges from 300 to 320 mOsm/kg. Usually, 90 mL of space is created in the intracranial vault by 1.6% reduction in brain water content. Osmotherapy has cerebral dehydrating effects. The main goal of osmotherapy is to decrease intracranial pressure (ICP) by shifting excess fluid from brain. This is accomplished by intravenous administration of osmotic agents which increase serum osmolality in order to shift excess fluid from intracellular or extracellular space of the brain to intravascular compartment. The resulting brain shrinkage effectively reduces intracranial volume and decreases ICP.
Autoregulation is a process within many biological systems, resulting from an internal adaptive mechanism that works to adjust that system's response to stimuli. While most systems of the body show some degree of autoregulation, it is most clearly observed in the kidney, the heart, and the brain. Perfusion of these organs is essential for life, and through autoregulation the body can divert blood where it is most needed.

Neurocritical care is a medical field that treats life-threatening diseases of the nervous system and identifies, prevents, and treats secondary brain injury.

An external ventricular drain (EVD), also known as a ventriculostomy or extraventricular drain, is a device used in neurosurgery to treat hydrocephalus and relieve elevated intracranial pressure when the normal flow of cerebrospinal fluid (CSF) inside the brain is obstructed. An EVD is a flexible plastic catheter placed by a neurosurgeon or neurointensivist and managed by intensive care unit (ICU) physicians and nurses. The purpose of external ventricular drainage is to divert fluid from the ventricles of the brain and allow for monitoring of intracranial pressure. An EVD must be placed in a center with full neurosurgical capabilities, because immediate neurosurgical intervention can be needed if a complication of EVD placement, such as bleeding, is encountered.
The monitoring of intracranial pressure (ICP) is used in the treatment of a number of neurological conditions ranging from severe traumatic brain injury to stroke and brain bleeds. This process is called intracranial pressure monitoring. Monitoring is important as persistent increases in ICP is associated with worse prognosis in brain injuries due to decreased oxygen delivery to the injured area and risk of brain herniation.
Increased intracranial pressure (ICP) is one of the major causes of secondary brain ischemia that accompanies a variety of pathological conditions, most notably traumatic brain injury (TBI), strokes, and intracranial hemorrhages. It can cause complications such as vision impairment due to intracranial pressure (VIIP), permanent neurological problems, reversible neurological problems, seizures, stroke, and death. However, aside from a few Level I trauma centers, ICP monitoring is rarely a part of the clinical management of patients with these conditions. The infrequency of ICP can be attributed to the invasive nature of the standard monitoring methods. Additional risks presented to patients can include high costs associated with an ICP sensor's implantation procedure, and the limited access to trained personnel, e.g. a neurosurgeon. Alternative, non-invasive measurement of intracranial pressure, non-invasive methods for estimating ICP have, as a result, been sought.
Cerebral autoregulation is a process in mammals that aims to maintain adequate and stable cerebral blood flow. While most systems of the body show some degree of autoregulation, the brain is very sensitive to over- and underperfusion. Cerebral autoregulation plays an important role in maintaining an appropriate blood flow to that region. Brain perfusion is essential for life, since the brain has a high metabolic demand. By means of cerebral autoregulation, the body is able to deliver sufficient blood containing oxygen and nutrients to the brain tissue for this metabolic need, and remove CO2 and other waste products.

Spaceflight-associated neuro-ocular syndrome (SANS), previously called spaceflight-induced visual impairment, is hypothesized to be a result of increased intracranial pressure (ICP), although, experiments directly measuring ICP in parabolic flight have shown ICP to be in normal physiological ranges during acute weightless exposure. The study of visual changes and ICP in astronauts on long-duration flights is a relatively recent topic of interest to space medicine professionals. Although reported signs and symptoms have not appeared to be severe enough to cause blindness in the near term, long term consequences of chronically elevated intracranial pressure are unknown.
John Douglas Pickard is a British professor emeritus of neurosurgery in the Department of Clinical Neurosciences of University of Cambridge. He is the honorary director of the National Institute for Health Research (NIHR) Healthcare Technology Cooperative (HTC) for brain injury. His research focuses on advancing the care of patients with acute brain injury, hydrocephalus and prolonged disorders of consciousness through functional brain imaging, studies of pathophysiology and new treatments; as well as focusing on health, economic and ethical aspects.
Clinicians routinely check the pupils of critically injured and ill patients to monitor neurological status. However, manual pupil measurements have been shown to be subjective, inaccurate, and not repeatable or consistent. Automated assessment of the pupillary light reflex has emerged as an objective means of measuring pupillary reactivity across a range of neurological diseases, including stroke, traumatic brain injury and edema, tumoral herniation syndromes, and sports or war injuries. Automated pupillometers are used to assess an array of objective pupillary variables including size, constriction velocity, latency, and dilation velocity, which are normalized and standardized to compute an indexed score such as the Neurological Pupil index (NPi).