| Anterior compartment syndrome of the lower leg | |
|---|---|
| Specialty | Rheumatology |
A compartment syndrome is an increased pressure within a muscular compartment [1] that compromises the circulation to the muscles.
| Anterior compartment syndrome of the lower leg | |
|---|---|
| Specialty | Rheumatology |
A compartment syndrome is an increased pressure within a muscular compartment [1] that compromises the circulation to the muscles.
Diffuse tightness and tenderness over the entire belly of the tibialis anterior muscle that does not respond to elevation or pain medication can be early warning signs and suggestive of Anterior Compartment Syndrome. Other common symptoms include excessive swelling that causes the skin to become hot, stretched and glossy. Pain, paresthesias, and tenderness in both the ischemic muscles and the region supplied by the deep common fibular nerve are exhibited by patients with this condition. Sensitivity to passive stretch and active contraction are common, and tend to increase the symptoms.[ citation needed ]
A compartment space is anatomically determined by an unyielding fascial (and osseous) enclosure of the muscles. The anterior compartment syndrome of the lower leg (often referred to simply as anterior compartment syndrome), can affect any and all four muscles of that compartment: tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius.[ citation needed ]
This term is often mistakenly used to describe various related/proximal conditions, including Anterior Shin Splints. It is important to distinguish between the two, as shin splints rarely causes serious health problems, while Anterior Compartment Syndrome can lead to irreversible damage.[ citation needed ]
The true compartment syndrome arises due to increased pressure within the unyielding anterior compartment of the leg. The pressure obstructs venous outflow, which causes further swelling and increased pressure. The resultant ischemia leads to necrosis (death of tissue) of the muscles and nerves. The process can begin with swelling of the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and/or the peroneus tertius muscles in response to strong eccentric contractions sufficient to produce postexercise soreness.[ citation needed ]
If these symptoms are observed/experienced it is important to contact a physician specializing in sports medicine (MD/DO), a doctor of podiatric medicine (DPM), or other qualified health care professional immediately so as to get the appropriate advice/treatment before serious damage occurs.[ citation needed ]
The 5 Ps of Anterior Compartment Syndrome:
The only option to treat acute compartment syndrome is surgery. The procedure, called a fasciotomy, involves a surgeon cutting open the skin and the fascia to relieve the pressure. Options to treat chronic compartment syndrome include physiotherapy, shoe inserts, and anti-inflammatory medications.[ citation needed ]

The foot is an anatomical structure found in many vertebrates. It is the terminal portion of a limb which bears weight and allows locomotion. In many animals with feet, the foot is a separate organ at the terminal part of the leg made up of one or more segments or bones, generally including claws or nails.

The human leg, in the general word sense, is the entire lower limb of the human body, including the foot, thigh and even the hip or gluteal region. However, the definition in human anatomy refers only to the section of the lower limb extending from the knee to the ankle, also known as the crus or, especially in non-technical use, the shank. Legs are used for standing, and all forms of locomotion including recreational such as dancing, and constitute a significant portion of a person's mass. Female legs generally have greater hip anteversion and tibiofemoral angles, but shorter femur and tibial lengths than those in males.

The sciatic nerve, also called the ischiadic nerve, is a large nerve in humans and other vertebrate animals which is the largest branch of the sacral plexus and runs alongside the hip joint and down the lower limb. It is the longest and widest single nerve in the human body, going from the top of the leg to the foot on the posterior aspect. The sciatic nerve has no cutaneous branches for the thigh. This nerve provides the connection to the nervous system for the skin of the lateral leg and the whole foot, the muscles of the back of the thigh, and those of the leg and foot. It is derived from spinal nerves L4 to S3. It contains fibers from both the anterior and posterior divisions of the lumbosacral plexus.

The extensor hallucis longus muscle is a thin skeletal muscle, situated between the tibialis anterior and the extensor digitorum longus. It extends the big toe and dorsiflects the foot. It also assists with foot eversion and inversion.
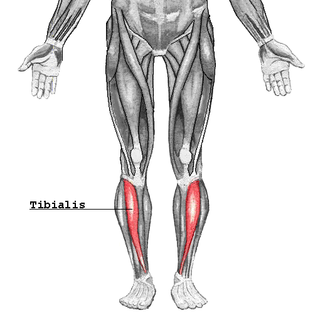
The tibialis anterior muscle is a muscle in humans that originates along the upper two-thirds of the lateral (outside) surface of the tibia and inserts into the medial cuneiform and first metatarsal bones of the foot. It acts to dorsiflex and invert the foot. This muscle is mostly located near the shin.

The flexor hallucis longus muscle (FHL) is one of the three deep muscles of the posterior compartment of the leg that attaches to the plantar surface of the distal phalanx of the great toe. The other deep muscles are the flexor digitorum longus and tibialis posterior; the tibialis posterior is the most powerful of these deep muscles. All three muscles are innervated by the tibial nerve which comprises half of the sciatic nerve.

The flexor digitorum longus muscle is situated on the tibial side of the leg. At its origin it is thin and pointed, but it gradually increases in size as it descends. It serves to flex the second, third, fourth, and fifth toes.
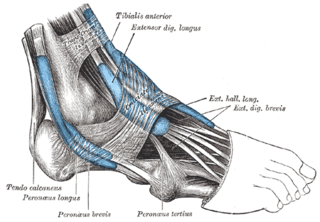
The extensor digitorum longus is a pennate muscle, situated at the lateral part of the front of the leg.

In human anatomy, the fibularis tertius is a muscle in the anterior compartment of the leg. It acts to tilt the sole of the foot away from the midline of the body (eversion) and to pull the foot upward toward the body (dorsiflexion).

The deep fibular nerve begins at the bifurcation of the common fibular nerve between the fibula and upper part of the fibularis longus, passes infero-medially, deep to the extensor digitorum longus, to the anterior surface of the interosseous membrane, and comes into relation with the anterior tibial artery above the middle of the leg; it then descends with the artery to the front of the ankle-joint, where it divides into a lateral and a medial terminal branch.

Foot drop is a gait abnormality in which the dropping of the forefoot happens due to weakness, irritation or damage to the deep fibular nerve, including the sciatic nerve, or paralysis of the muscles in the anterior portion of the lower leg. It is usually a symptom of a greater problem, not a disease in itself. Foot drop is characterized by inability or impaired ability to raise the toes or raise the foot from the ankle (dorsiflexion). Foot drop may be temporary or permanent, depending on the extent of muscle weakness or paralysis and it can occur in one or both feet. In walking, the raised leg is slightly bent at the knee to prevent the foot from dragging along the ground.

The sole is the bottom of the foot.
The inferior extensor retinaculum of the foot is a Y-shaped band placed in front of the ankle-joint, the stem of the Y being attached laterally to the upper surface of the calcaneus, in front of the depression for the interosseous talocalcaneal ligament; it is directed medialward as a double layer, one lamina passing in front of, and the other behind, the tendons of the peroneus tertius and extensor digitorum longus.

The fibularis muscles are a group of muscles in the lower leg.

The interosseous membrane of the leg extends between the interosseous crests of the tibia and fibula, helps stabilize the Tib-Fib relationship and separates the muscles on the front from those on the back of the leg.
The superior extensor retinaculum of the foot is the upper part of the extensor retinaculum of foot which extends from the ankle to the heelbone.
The posterior compartment of the forearm contains twelve muscles which are chiefly responsible for extension of the wrist and digits, and supination of the forearm. It is separated from the anterior compartment by the interosseous membrane between the radius and ulna.

The anterior compartment of the leg is a fascial compartment of the lower [leg]. It contains muscles that produce dorsiflexion and participate in inversion and eversion of the foot, as well as vascular and nervous elements, including the anterior tibial artery and veins and the deep fibular nerve.