
Dizziness is an imprecise term that can refer to a sense of disorientation in space, vertigo, or lightheadedness. It can also refer to disequilibrium or a non-specific feeling, such as giddiness or foolishness.

A gait is a manner of limb movements made during locomotion. Human gaits are the various ways in which humans can move, either naturally or as a result of specialized training. Human gait is defined as bipedal forward propulsion of the center of gravity of the human body, in which there are sinuous movements of different segments of the body with little energy spent. Varied gaits are characterized by differences such as limb movement patterns, overall velocity, forces, kinetic and potential energy cycles, and changes in contact with the ground.

Labyrinthitis is inflammation of the labyrinth, a maze of fluid-filled channels in the inner ear. Vestibular neuritis is inflammation of the vestibular nerve. Both conditions involve inflammation of the inner ear. Labyrinths that house the vestibular system sense changes in the head's position or the head's motion. Inflammation of these inner ear parts results in a sensation of the world spinning and also possible hearing loss or ringing in the ears. It can occur as a single attack, a series of attacks, or a persistent condition that diminishes over three to six weeks. It may be associated with nausea, vomiting, and eye nystagmus.

The motion aftereffect (MAE) is a visual illusion experienced after viewing a moving visual stimulus for a time with stationary eyes, and then fixating a stationary stimulus. The stationary stimulus appears to move in the opposite direction to the original stimulus. The motion aftereffect is believed to be the result of motion adaptation.

Vertigo is a condition in which a person has the sensation of movement or of surrounding objects moving when they are not. Often it feels like a spinning or swaying movement. It may be associated with nausea, vomiting, perspiration, or difficulties walking. It is typically worse when the head is moved. Vertigo is the most common type of dizziness.
Romberg's test, Romberg's sign, or the Romberg maneuver is a test used in an exam of neurological function for balance. The exam is based on the premise that a person requires at least two of the three following senses to maintain balance while standing: proprioception ; vestibular function ; and vision.

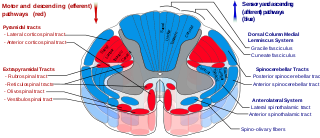
The vestibulospinal tract is a neural tract in the central nervous system. Specifically, it is a component of the extrapyramidal system and is classified as a component of the medial pathway. Like other descending motor pathways, the vestibulospinal fibers of the tract relay information from nuclei to motor neurons. The vestibular nuclei receive information through the vestibulocochlear nerve about changes in the orientation of the head. The nuclei relay motor commands through the vestibulospinal tract. The function of these motor commands is to alter muscle tone, extend, and change the position of the limbs and head with the goal of supporting posture and maintaining balance of the body and head.

Balance in biomechanics, is an ability to maintain the line of gravity of a body within the base of support with minimal postural sway. Sway is the horizontal movement of the centre of gravity even when a person is standing still. A certain amount of sway is essential and inevitable due to small perturbations within the body or from external triggers. An increase in sway is not necessarily an indicator of dysfunctional balance so much as it is an indicator of decreased sensorimotor control.

Illusions of self-motion occur when one perceives bodily motion despite no movement taking place. One can experience illusory movements of the whole body or of individual body parts, such as arms or legs.

The evolution of human bipedalism, which began in primates approximately four million years ago, or as early as seven million years ago with Sahelanthropus, or approximately twelve million years ago with Danuvius guggenmosi, has led to morphological alterations to the human skeleton including changes to the arrangement, shape, and size of the bones of the foot, hip, knee, leg, and the vertebral column. These changes allowed for the upright gait to be overall more energy efficient in comparison to quadrupeds. The evolutionary factors that produced these changes have been the subject of several theories that correspond with environmental changes on a global scale.

Blocq's disease was first considered by Paul Blocq (1860–1896), who described this phenomenon as the loss of memory of specialized movements causing the inability to maintain an upright posture, despite normal function of the legs in the bed. The patient is able to stand up, but as soon as the feet are on the ground, the patient cannot hold himself upright nor walk; however when lying down, the subject conserved the integrity of muscular force and the precision of movements of the lower limbs. The motivation of this study came when a fellow student Georges Marinesco (1864) and Paul published a case of parkinsonian tremor (1893) due to a tumor located in the substantia nigra.

Locomotor effects of shoes are the way in which the physical characteristics or components of shoes influence the locomotion neuromechanics of a person. Depending on the characteristics of the shoes, the effects are various, ranging from alteration in balance and posture, muscle activity of different muscles as measured by electromyography (EMG), and the impact force. There are many different types of shoes that exist, such as running, walking, loafers, high heels, sandals, slippers, work boots, dress shoes, and many more. However, a typical shoe will be composed of an insole, midsole, outsole, and heels, if any. In an unshod condition, where one is without any shoes, the locomotor effects are primarily observed in the heel strike patterns and resulting impact forces generated on the ground.

Spinal locomotion results from intricate dynamic interactions between a central program in lower thoracolumbar spine and proprioceptive feedback from body in the absence of central control by brain as in complete spinal cord injury (SCI). Following SCI, the spinal circuitry below the lesion site does not become silent; rather, it continues to maintain active and functional neuronal properties, although in a modified manner.

Parkinsonian gait is the type of gait exhibited by patients with Parkinson's disease (PD). It is often described by people with Parkinson's as feeling like being stuck in place, when initiating a step or turning, and can increase the risk of falling. This disorder is caused by a deficiency of dopamine in the basal ganglia circuit leading to motor deficits. Gait is one of the most affected motor characteristics of this disorder although symptoms of Parkinson's disease are varied.
A gait trainer is a wheeled device that assists a person who is unable to walk independently to learn or relearn to walk safely and efficiently as part of gait training. Gait trainers are intended for children or adults with physical disabilities, to provide the opportunity to improve walking ability. A gait trainer offers both unweighting support and postural alignment to enable gait practice. It functions as a support walker and provides more assistance for balance and weight-bearing, than does a traditional rollator walker, or a walker with platform attachments. It also provides opportunities to stand and to bear weight in a safe, supported position.

The fear of falling (FOF), also referred to as basophobia, is a natural fear and is typical of most humans and mammals, in varying degrees of extremity. It differs from acrophobia, although the two fears are closely related. The fear of falling encompasses the anxieties accompanying the sensation and the possibly dangerous effects of falling, as opposed to the heights themselves. Those who have little fear of falling may be said to have a head for heights. Basophobia is sometimes associated with astasia-abasia, the fear of walking/standing erect.
The term chronic subjective dizziness (CSD) is used to describe a commonly encountered type of dizziness that is not easily categorized into one of several other types, and for which the physical examination is typically normal. Patients with CSD frequently initially suffer a sudden injury of some sort to their vestibular system, the neurologic network that preserves sense of balance. Even after this initial injury has healed, people with CSD usually describe a vague sense of unsteadiness worsened by triggers in their environment such as high places, standing on moving objects, or standing in motion-rich environments like busy streets or crowds. There is a clear indication that anxiety and other mental illnesses play a role in the dizziness symptoms that occur with CSD. However, the condition is categorized as chronic functional vestibular disorder, not as a structural or psychiatric condition.
The mesencephalic locomotor region (MLR) is a functionally defined area of the midbrain that is associated with the initiation and control of locomotor movements in vertebrate species.

Gait deviations are nominally referred to as any variation of standard human gait, typically manifesting as a coping mechanism in response to an anatomical impairment. Lower-limb amputees are unable to maintain the characteristic walking patterns of an able-bodied individual due to the removal of some portion of the impaired leg. Without the anatomical structure and neuromechanical control of the removed leg segment, amputees must use alternative compensatory strategies to walk efficiently. Prosthetic limbs provide support to the user and more advanced models attempt to mimic the function of the missing anatomy, including biomechanically controlled ankle and knee joints. However, amputees still display quantifiable differences in many measures of ambulation when compared to able-bodied individuals. Several common observations are whole-body movements, slower and wider steps, shorter strides, and increased sway.
Gait variability seen in Parkinson's Disorders arise due to cortical changes induced by pathophysiology of the disease process. Gait rehabilitation is focused to harness the adapted connections involved actively to control these variations during the disease progression. Gait variabilities seen are attributed to the defective inputs from the Basal Ganglia. However, there is altered activation of other cortical areas that support the deficient control to bring about a movement and maintain some functional mobility.
