Related Research Articles
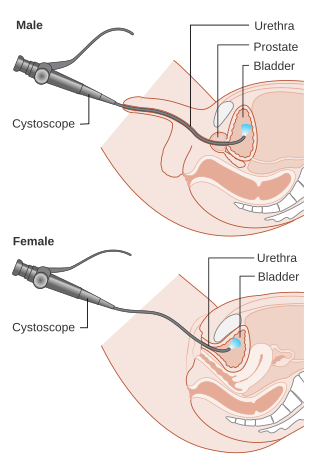
Cystoscopy is endoscopy of the urinary bladder via the urethra. It is carried out with a cystoscope.
Urinary incontinence (UI), also known as involuntary urination, is any uncontrolled leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. It has been identified as an important issue in geriatric health care. The term enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis. UI is an example of a stigmatized medical condition, which creates barriers to successful management and makes the problem worse. People may be too embarrassed to seek medical help, and attempt to self-manage the symptom in secrecy from others.

In urinary catheterization, a latex, polyurethane, or silicone tube known as a urinary catheter is inserted into the bladder through the urethra to allow urine to drain from the bladder for collection. It may also be used to inject liquids used for treatment or diagnosis of bladder conditions. A clinician, often a nurse, usually performs the procedure, but self-catheterization is also possible. A catheter may be in place for long periods of time or removed after each use.

A colostomy is an opening (stoma) in the large intestine (colon), or the surgical procedure that creates one. The opening is formed by drawing the healthy end of the colon through an incision in the anterior abdominal wall and suturing it into place. This opening, often in conjunction with an attached ostomy system, provides an alternative channel for feces to leave the body. Thus if the natural anus is unavailable for that function, an artificial anus takes over. It may be reversible or irreversible, depending on the circumstances.

Urinary retention is an inability to completely empty the bladder. Onset can be sudden or gradual. When of sudden onset, symptoms include an inability to urinate and lower abdominal pain. When of gradual onset, symptoms may include loss of bladder control, mild lower abdominal pain, and a weak urine stream. Those with long-term problems are at risk of urinary tract infections.
In anatomy, a stoma is any opening in the body. For example, a mouth, a nose, and an anus are natural stomata. Any hollow organ can be manipulated into an artificial stoma as necessary. This includes the esophagus, stomach, duodenum, ileum, colon, pleural cavity, ureters, urinary bladder, and renal pelvis. Such a stoma may be permanent or temporary.

Ileostomy is a stoma constructed by bringing the end or loop of small intestine out onto the surface of the skin, or the surgical procedure which creates this opening. Intestinal waste passes out of the ileostomy and is collected in an external ostomy system which is placed next to the opening. Ileostomies are usually sited above the groin on the right hand side of the abdomen.

In urology, a Foley catheter is one of many types of urinary catheters (UC). The Foley UC was named after Frederic Foley, who produced the original design in 1929. Foleys are indwelling UC, often referred to as an IDCs. This differs from in/out catheters. The UC is a flexible tube if it is indwelling and stays put, or rigid if it is in/out, that a clinician, or the client themselves, often in the case of in/out UC, passes it through the urethra and into the bladder to drain urine.

Cystectomy is a medical term for surgical removal of all or part of the urinary bladder. It may also be rarely used to refer to the removal of a cyst. The most common condition warranting removal of the urinary bladder is bladder cancer.

A urostomy is a surgical procedure that creates a stoma for the urinary system. A urostomy is made to avail for urinary diversion in cases where drainage of urine through the bladder and urethra is not possible, e.g. after extensive surgery or in case of obstruction.

The Mitrofanoff procedure, also known as the Mitrofanoff appendicovesicostomy, is a surgical procedure in which the appendix is used to create a conduit, or channel, between the skin surface and the urinary bladder. The small opening on the skin surface, or the stoma, is typically located either in the navel or nearby the navel on the right lower side of the abdomen. Originally developed by Professor Paul Mitrofanoff in 1980, the procedure represents an alternative to urethral catheterization and is sometimes used by people with urethral damage or by those with severe autonomic dysreflexia. An intermittent catheter, or a catheter that is inserted and then removed after use, is typically passed through the channel every 3–4 hours and the urine is drained into a toilet or a bottle. As the bladder fills, rising pressure compresses the channel against the bladder wall, creating a one-way valve that prevents leakage of urine between catheterizations.

A suprapubic cystostomy or suprapubic catheter (SPC) is a surgically created connection between the urinary bladder and the skin used to drain urine from the bladder in individuals with obstruction of normal urinary flow. The connection does not go through the abdominal cavity.

An ileal conduit urinary diversion is one of various surgical techniques for urinary diversion. It has sometimes been referred to as the Bricker ileal conduit after its inventor, Eugene M. Bricker. It is a form of incontinent urostomy, and was developed during the 1940s and is still one of the most used techniques for the diversion of urine after a patient has had their bladder removed, due to its low complication rate and high patient satisfaction level. It is usually used in conjunction with radical cystectomy in order to control invasive bladder cancer.

Posterior urethral valve (PUV) disorder is an obstructive developmental anomaly in the urethra and genitourinary system of male newborns. A posterior urethral valve is an obstructing membrane in the posterior male urethra as a result of abnormal in utero development. It is the most common cause of bladder outlet obstruction in male newborns. The disorder varies in degree, with mild cases presenting late due to milder symptoms. More severe cases can have renal and respiratory failure from lung underdevelopment as result of low amniotic fluid volumes, requiring intensive care and close monitoring. It occurs in about one in 8,000 babies.

A ureteral stent, or ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 and 30 cm. Additionally, stents come in differing diameters or gauges, to fit different size ureters. The stent is usually inserted with the aid of a cystoscope. One or both ends of the stent may be coiled to prevent it from moving out of place; this is called a JJ stent, double J stent or pig-tail stent.
Urinary diversion is any one of several surgical procedures to reroute urine flow from its normal pathway. It may be necessary for diseased or defective ureters, bladder or urethra, either temporarily or permanently. Some diversions result in a stoma.
A urine collection device or UCD is a device that allows the collection of urine for analysis or for purposes of simple elimination. UCDs of the latter type are sometimes called piddle packs.
Neurogenic bladder dysfunction, often called by the shortened term neurogenic bladder, refers to urinary bladder problems due to disease or injury of the central nervous system or peripheral nerves involved in the control of urination. There are multiple types of neurogenic bladder depending on the underlying cause and the symptoms. Symptoms include overactive bladder, urinary urgency, frequency, incontinence or difficulty passing urine. A range of diseases or conditions can cause neurogenic bladder including spinal cord injury, multiple sclerosis, stroke, brain injury, spina bifida, peripheral nerve damage, Parkinson's disease, multiple system atrophy or other neurodegenerative diseases. Neurogenic bladder can be diagnosed through a history and physical as well as imaging and more specialized testing. In addition to symptomatic treatment, treatment depends on the nature of the underlying disease and can be managed with behavioral changes, medications, surgeries, or other procedures. The symptoms of neurogenic bladder, especially incontinence, can severely degrade a person's quality of life.

A ureterostomy is the creation of a stoma for a ureter or kidney.
Nils G. Kock was a professor of surgery who taught and practiced at the University of Gothenburg, Gothenburg, Sweden. Kock was noted for his research, experimentation, and colorectal surgical techniques. These led to his breakthrough development of the Kock pouch, used for people who require excretory stomas.
References
- ↑ Rowland RG; Mitchell ME; Bihrle R; Kahnoski RJ; Piser JE (1987), "Indiana continent urinary reservoir", Journal of Urology, 137 (6): 1136–1139, doi:10.1016/s0022-5347(17)44428-4, PMID 3586143
- ↑ "Bard Medical". www.bardmedical.com. Archived from the original on 2018-07-08. Retrieved 2016-07-26.
- ↑ Van Der Aa, Frank; Joniau, Steven; Van Den Branden, Marcel; Van Poppel, Hein (2011). "Metabolic Changes after Urinary Diversion". Advances in Urology. 2011: 1–5. doi: 10.1155/2011/764325 . PMC 3113422 . PMID 21687576.